Infectious-toxic shock is a nonspecific pathological condition caused by the influence of bacteria and the toxins they secrete. This process can be accompanied by various disorders - metabolic, neuroregulatory and hemodynamic. This condition of the human body is an emergency and requires immediate treatment. The disease can affect absolutely anyone, regardless of gender and age group. In the international classification of diseases (ICD 10), toxic shock syndrome has its own code - A48.3.
Do not self-medicate. At the first signs of illness, consult a doctor.
- Etiology
- Varieties
- Symptoms
- Complications
- Diagnostics
- Treatment
- Prevention
The cause of this disease is severe infectious processes. Infectious-toxic shock in children is often formed on the basis of pneumonia. The development of such a syndrome depends entirely on the causative agent of this disease, the state of the person’s immune system, the presence or absence of drug therapy, and the intensity of exposure to the bacterium.
The characteristic symptoms of the disease are a combination of signs of acute circulatory failure and a massive inflammatory process. Often the external expression develops quite quickly, especially in the first few days of progression of the underlying disease. The very first symptom is severe chills. A little later, increased sweating, intense headaches, convulsions, and episodes of loss of consciousness appear. In children, this syndrome manifests itself somewhat differently - frequent vomiting that has nothing to do with eating, diarrhea and a gradual increase in pain.
Diagnosis of infectious-toxic shock consists of detecting the pathogen in the patient's blood tests. Treatment of the disease is based on the use of medications and special solutions. Since this syndrome is a very serious condition, before the patient enters a medical facility, he must be given first aid. The prognosis of toxic shock syndrome is relatively favorable and depends on timely diagnosis and effective treatment tactics. However, the chance of death is forty percent.
General information
The term “shock” is a collective concept used to characterize special (urgent) conditions of the body’s most important vital functions, manifested by a complex of pathological processes resulting from extreme exposure to various factors.
An emergency condition of the body that occurs as a result of bacteremia, caused both by the action of the bacteria themselves and by their biologically active substances (exo/endotoxins), is called infectious toxic shock (ITSH). It is based on a complex of pathological disorders of the vital functions of the body, caused by inadequate or excessive compensatory reactions, manifested by disorders of blood circulation, respiration, blood coagulation, endocrine regulation, metabolic disorders, and central nervous system function, leading to the development of multiple organ failure. Despite the achievements of modern medicine, ITS is a common syndrome that causes the emergency condition of patients admitted to the intensive care unit/infectious diseases hospital.
The importance of timely diagnosis and treatment of ITS remains a pressing problem to this day, since such conditions are accompanied by high mortality rates (25-30%). In terms of incidence, ITS ranks third after cardiogenic and hemorrhagic shock , and in terms of mortality - first.
ITS is a serious complication of a number of infectious diseases accompanied by persistently severe bacteremia. The most common infectious-toxic shock is pneumonia (lobar), especially pneumonia caused by pneumococci ; meningococcemia ; typhoid and typhus , salmonellosis ; hemorrhagic fevers ; shigellosis ; plague; hypertoxic form of diphtheria . Quite often, bacteremic (endotoxic) shock occurs with septic complications in various purulent diseases, postpartum complications, abortion , and inflammatory diseases of the urinary tract. It can also develop against the background of other infectious diseases with unreasonably large doses of prescribed antibiotics.
In the 80s of the last century, cases of the development of ITS when using vaginal tampons were first described. Infectious-toxic shock from tampons (menstrual toxic shock syndrome) in most cases develops as a result of long-term use of super-absorbent hygienic tampons, diaphragms and caps, which creates favorable conditions for the development of microflora and the production of toxins . It is most often caused by exotoxin-producing bacteria - group A pyogenic β-hemolytic streptococcus and Staphylococcus aureus. At the same time, endotoxic shock most often occurs against the background of chronic carriage of pathogens, and improper use of tampons (failure to replace them on time) is a predisposing factor that creates favorable conditions for the proliferation of microorganisms and their penetration into the blood.
Varieties
There is a classification of toxic shock syndrome depending on the degree of its development. This division is based on the severity of symptoms. Thus, we distinguish:
- initial degree - in which blood pressure remains unchanged, but heart rate increases. It can reach one hundred and twenty beats per minute;
- moderate severity – characterized by progression of symptoms from the cardiovascular system. Accompanied by a decrease in systolic blood pressure and increased heart rate;
- severe degree - a significant drop in systolic tone (pressure reaches seventy millimeters of mercury). The shock index increases. Fever and a decrease in the volume of urine emitted are often observed;
- complicated stage – characterized by the development of irreversible changes in internal organs and tissues. The patient's skin takes on an earthy tint. A comatose state is often observed.
Depending on the pathogen, there are:
- streptococcal syndrome - occurs after childbirth, infection of wounds, cuts or burns of the skin, and is also a complication after infectious disorders, in particular pneumonia;
- staphylococcal toxic shock - often develops after surgery and the use of hygienic tampons;
- bacterial toxic shock - occurs due to blood poisoning and can complicate any stage of sepsis.
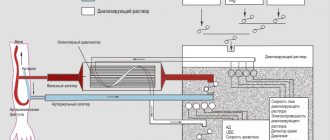
Pathogenesis
The mechanism of the damaging effect of ITS is quite complex and is determined primarily by the pathogenicity factors of the pathogen, which are individual for each type of bacteria. Thus, Salmonella has significantly fewer aggressive factors, and their shockogenic properties are weaker than those of the plague pathogen. The likelihood of developing ITS is determined both by the pathogenic properties of the pathogen and the state of the human immune system in whose body these pathological processes develop. The main interaction between external and internal factors occurs primarily in the microvasculature, the pathological changes of which predetermine the development of ITS in the future. The triggering factor for the cascade development of reactions is the entry into the blood of a large number of bacteria and bacterial toxins.
The basis of the endotoxin of gram-negative bacteria is the somatic antigen lipopolysaccharide (LPS). Endotoxin is released predominantly only after the death of the bacterial cell and exhibits pronounced biological activity. The toxic effect of LPS is based on massive stimulation of cells of the lymphoreticular system, promoting the release in large volumes of cytokines and other mediators of the inflammatory response and shock. It is they who, in ITS, play a critical role in the appearance of fever, tissue damage, and the development of severe arterial hypotension . LPS also have direct cardiodepressive and cytotoxic effects. ITS is developing relatively quickly.
Most gram-positive bacteria do not contain endotoxin, but have a liposaccharide capsule and specific antigens (including exotoxins). Such components of the bacterial cell stimulate the production of cytokines and change the activity of lymphocytes/mononuclear macrophages, so their action is to a certain extent determined by humoral factors.
The combination of aggressive factors causes a predominance of pro-inflammatory factors, which forms the systemic inflammatory response syndrome, which is the pathogenetic basis of infectious-toxic shock.
Under the influence of a complex of damaging factors, a cascade of pathological reactions is triggered (vasodilation develops, vascular permeability increases, blood cell aggregation is activated and active lysosomal enzymes and oxygen radicals enter the blood), leading to metabolic , microcirculation, damage to vascular endothelial cells and blood elements, and increased permeability capillaries.
Against this background, the total peripheral vascular resistance in the microvasculature decreases and the volume of blood supply decreases significantly. A spasm of pre/postcapillaries is formed, arteriovenous shunts open, which leads to the flow of blood from the arterial bed into the venous bed, bypassing the capillary network. Myocardial contractility is inhibited. As a compensatory response, the production of adrenocorticotropic hormone , aldosterone and cortisol , which temporarily optimizes hemodynamics. However, further deterioration of microcirculation contributes to the formation of progressive hypoxia . It is microcirculation disorders and tissue hypoxia that determine the further progression of ITS - redistribution of systemic blood flow, retention of water and salts by the kidneys, transfer of interstitial fluid from tissues to blood vessels, increased blood glucose levels, and increased myocardial work.
Effective therapeutic measures taken at this stage to eliminate the causes of ITS make it possible to restore microcirculation and circulating blood volume (CBV) in full, thereby stopping the development of the pathological process. In cases of insufficiency/ineffectiveness of therapeutic measures and with the continued entry of toxic agents into the blood, the development of ITS continues.
The onset of rheological disorders worsen, DIC and sludge syndrome develop, acidosis in tissues worsens, tissue metabolites accumulate, causing expansion of the precapillaries while the postcapillaries remain spasmodic. At the same time, blood is pumped into the microvasculature with increased permeability (depositing up to 10% of the bcc), which contributes to the exudation of serum proteins and blood plasma into the extravascular space and, accordingly, additional losses of circulating blood volume. Against this background, blood circulation is centralized so that vital organs (brain, heart, liver) receive it first.
In a state of tissue hypoxia and deep acidosis , blood circulation significantly worsens and all vascular reactions change, intracellular potassium is replaced by sodium, which causes cellular hyperhydration and fluid leaving the intravascular bed. Further, aggregation of blood elements, microthrombosis of blood vessels develop and peripheral blood circulation is practically blocked, coagulation is disrupted, irreversible degenerative changes occur in tissues and organs and multiple organ failure develops.
Against this background heart failure , severe shortness of breath , inhibition of various parts of the central nervous system, including the vasomotor center, increases, cerebral edema , interstitial pulmonary edema , oliguria begins, cardiac and respiratory reflexes are inhibited, disturbances of consciousness appear and often end in death. The causes of death are irreversible multiple organ failure (50%), severe arterial hypotension (40%), and decompensated heart failure (10%).
Classification
There is a reversible ITS, which includes 3 stages:
- Early reversible - characterized by spasm in the microvasculature and with initial symptoms of tissue hypoxia.
- Late reversible - characterized by expansion of the microcirculatory bed with the deposition of blood in it; increased hypoxia, initial control of enzymatic metabolism in the tissues of the most sensitive organs.
- Sustained reversible (decompensated shock) - development of disseminated intravascular coagulation (stage 1-2), severe hypoxia, signs of dysfunction of individual organs.
Irreversible ITS is DIC syndrome (stage 3-4) with severe disorders of microcirculation and blood coagulation. Severe intracellular acidosis. Symptoms of irreversible multiple organ failure.
Causes
The most common cause of the development of ITS are gram-negative enterobacteria (70% of cases) - pneumococcus , Escherichia coli , salmonella , meningococcus , Proteus , Klebsiella , Pseudomonas aeruginosa . Less commonly - gram-positive microflora - enterococci , streptococci , staphylococci or viruses (herpes, CMV), protozoa, fungi.
In addition to the presence of an infectious agent in the body, the development of ITS requires a combination of two additional factors:
- Opportunities for massive penetration of the pathogen and/or its toxins into the bloodstream.
- Reducing the general resistance (immunodeficiency) of the body.
Risk factors for the development of ICT are:
- Incorrect antibiotic .
- Complicated abortion/puerperal sepsis .
- Diseases of the ENT organs (sinusitis, tracheitis), closed wounds (in the nose).
- Open wounds, burns .
- Postoperative purulent complications.
- Improper use of tampons during menstruation and means of preventing pregnancy (intravaginal contraceptives - diaphragms/caps).
- Immunodeficiency states of the body.
Treatment
Before carrying out therapy in a medical facility, it is necessary to provide the patient with emergency first aid. Such events consist of several stages, which include:
- ridding the victim of narrow and tight clothing;
- ensuring a horizontal position so that the head is slightly elevated in relation to the entire body;
- You need to put a heating pad under your feet;
- allow fresh air to flow in.
These actions are limited to emergency care, which is not performed by a specialist.
After transporting the patient to a medical facility, intensive treatment of infectious-toxic shock with medications begins. Often, hormonal substances, antibiotics and glucocorticoids are used to actively destroy bacteria. The use of medications is individual and depends on the causative agent of the disease.
If the infection occurs due to the use of tampons or vaginal contraceptives, then treatment is to immediately remove them from the body. This may require curettage, and the cavity is treated with antiseptic drugs.
Symptoms of toxic shock syndrome
Clinical symptoms of ICT include symptoms of acute circulatory failure and generalized infection. Specific manifestations are determined by the stage of development of the pathological process.
Stage 1.1. The phase of early reversible shock is not always clinically diagnosed and is short-lived. It is characterized by spasm in the microvasculature with initial manifestations of tissue hypoxia with the development of symptoms of peripheral vasodilation and a hyperdynamic state, which are manifested by anxiety. Pronounced motor and speech excitement, moderate thirst.
Vascular tone is not affected; sometimes there is generalized arteriolospasm , which causes pallor of the skin and mucous membranes. The skin is warm to the touch, sometimes moist. The pupils are constricted, breathing is rhythmic and deep, but against the background of fever it can become more frequent. The pulse rate is rapid, the pulse is tense, the blood pressure level is normal or slightly elevated. Diuresis is slightly reduced (hourly urine output is at least 40 ml/h). In the blood - hypercoagulation , hyperglycemia , slight metabolic acidosis . As already indicated, the vast majority of doctors almost never diagnose this phase.
Starting from stage 1.2 , a gradual decrease in cardiac output, an increase in spasm of peripheral vessels and the beginning of the functioning of arteriovenous shunts are characteristic. Tachycardia increases , blood pressure decreases (systolic blood pressure is below the level of 70-60 mm Hg, at which renal filtration almost stops and hypoxia of the kidney tissue increases).
In the absence of adequate medical care, the countdown of time begins from this stage, the duration of which subsequently determines the potential possibility of removing the patient from shock. The pulse is frequent (over 100 beats/min) and weak, heart sounds are muffled, breathing is rapid, severe lethargy and apathy. The pallor of the skin increases, it becomes cold and damp, acquires a marbled tint, acrocyanosis , and the facial skin has a gray-cyanotic color.
Stage 1.3 . Characterized by a further slowdown in capillary blood flow, an increase in hypovolemia , the development of disseminated intravascular coagulation syndrome, metabolic disorders, and inhibition of the sympathetic nervous system. Breathing in the lungs is harsh, and obvious increasing shortness of breath develops (respiratory rate more than 30/min). Partial pressure sharply decreases (below 50 mm Hg), diuresis decreases, hypoxia/hypercapnia sharply increases, cyanosis of the skin and mucous membranes increases, signs of multiple organ functional failure (pulmonary, renal and hepatic failure) appear, which is manifested by a decrease in urination (oliguria ), shortness of breath, jaundice.
Due to the progression of DIC syndrome (second stage), some patients develop a rash, often hemorrhagic in nature. Body temperature drops to subfebrile. The patient's condition is rapidly deteriorating, the pulse is soft and thready, there is severe tachycardia, and blood pressure may not be determined.
Irreversible shock phase - symptoms of systemic severe irreversible multiple organ failure develop: breathing is greatly accelerated, becomes shallow and ineffective (sometimes Cheyne-Stokes breathing). Signs of pulmonary edema appear - increasing moist rales, initially in the lower parts of the lungs, and then spreading to all the lungs. Severe cyanosis often becomes total. Body temperature reaches subnormal levels. brain hypoxia increase (a soporous state develops, turning into a coma). Subsequently, respiratory and cardiac activity stops. It should be noted that the symptoms of infectious toxic shock rapidly progress and it is not always possible to clinically clearly and timely differentiate all phases of ITS.
Symptoms of toxic shock syndrome from tampons appear more often on the 3rd-5th day of menstruation.
The disease begins acutely, and less often occurs with prodromal symptoms such as headache , general malaise, and nausea. The first sign of TSS is severe chills, the temperature rises to 39°C, after which full clinical symptoms develop over the course of 2-5 days. Most women experience diffuse muscle pain and muscle weakness, predominantly in the muscles of the proximal lower extremities, back and abdominals. Sometimes joint pain occurs. Characterized by persistent vomiting, watery diarrhea, decreased diuresis.
Dizziness, headache, paresthesia and fainting against the background of a sharp decrease in blood pressure. In the acute stage (the first 2 days), women are inhibited and partially disoriented. A specific manifestation of the syndrome is the appearance of skin rashes in the form of diffuse redness, spots or small nodular rashes, followed by peeling and peeling of the skin epithelium of the palms, fingers, toes, and soles. In 75% of patients, conjunctival hyperemia and redness of the mucous membrane and mouth of the posterior pharyngeal wall are detected. Most of them experience swelling in the area of the external genitalia and their soreness.
In the future, in the absence of treatment, symptoms of toxic damage to the respiratory and cardiovascular systems, liver, kidneys occur with shortness of breath, pain in the abdomen, right hypochondrium, lower back, and a sharp drop in blood pressure. Much less often, ITS from tampons occurs in a mild (erased) form. At the same time, against the background of chills , fever, nausea, vomiting, diarrhea and general malaise, blood pressure does not decrease, and the pathological condition often resolves without any treatment.
Diagnostics
Diagnostic measures for toxic shock syndrome are aimed at detecting the causative agent of the disease. Before performing laboratory and instrumental examinations of the patient, the doctor must carefully study the person’s medical history, determine the intensity of symptoms, and also conduct an examination. If the cause of this condition is the use of tampons, then patients are required to be examined by a gynecologist.
Other diagnostic methods include:
- conducting general and biochemical blood tests is the main way to identify the pathogen;
- measuring the amount of urine emitted per day - with such an illness, the volume of daily urine will be much less than that of a healthy person;
- instrumental examinations, which include CT, MRI, ultrasound, ECG, etc., aimed at determining the extent of damage to internal organs.
An experienced specialist can easily determine infectious-toxic shock by the patient’s appearance.
Tests and diagnostics
The main diagnostic criteria for ITS are the dynamics of indicators of the state of the cardiovascular and respiratory systems, blood parameters, and the diagnosis of metabolic disorders. General clinical methods for diagnosing stages of ITS are of secondary importance.
The diagnostic criteria for ITS are:
- Chills and hyperthermia (>38-39 °C), in the later stages paradoxical hypothermia (<36 °C).
- Microcirculation disorders (pale, cold skin).
- Hypoxemia / tachypnea (acrocyanosis, partial pressure <32 mm Hg; heart rate >20 per minute).
- Circulatory disorders (hypodynamic syndrome): Systolic blood pressure <90 mm Hg. tachycardia (heart rate 100-120/min) in the absence of other reasons for the development of hypotension. At the same time, infusion therapy does not restore hemodynamics.
- Neuropsychiatric disorders (euphoria, agitation, disorientation, stupor).
- Oligoanuria (less than 30 ml/h), diarrhea , vomiting.
- Blood parameters: accelerated ESR, leukocytosis (>12.0•109/l), neutrophilia >10%, LII >9; level of hematocrit, lactate (>2 mmol/l).
The diagnosis of ITS is made when there is a focus of infection in the body and two or more of the above symptoms.
Infectious-toxic shock in children
ITS in children is especially severe, with dynamically increasing symptoms. In addition to the listed diseases in adults, which are often complicated by ITS in children, it often develops against the background of dysentery , scarlet fever , diphtheria and meningococcal infection . Infectious-toxic shock is also often caused by the introduction of an infectious pathogen during scratches or scratching abrasions. The disease in children is characterized by active development of the process within 1-2 days. This is characterized by a sharp increase in body temperature to 39-41 C.
The child's condition is serious and is accompanied by severe chills, motor agitation, vomiting, convulsions, pallor of the mucous membranes and skin, increased heart rate, a significant and sharp drop in blood pressure, and confusion. With meningococcal infection, numerous hemorrhages of various shapes appear on the skin of children. Increasing microcirculation disorders can provoke an earlier development of acute renal failure .
Treatment of infectious-toxic shock in children should begin as quickly as possible and is carried out only in the intensive care unit according to a scheme similar to the treatment of ITS in adults with adjustment of drugs for the age/body weight of the child. Without adequate timely treatment, there is a high risk of death.
Complications
Quite often, people mistake the above symptoms for a cold or infection, which is why they are in no hurry to seek help from specialists. Without timely diagnosis and treatment, a number of irreversible complications of infectious-toxic shock may develop:
- impaired blood circulation, causing internal organs to not receive the proper amount of oxygen;
- acute respiratory failure – formed due to severe damage to the lungs, especially if the syndrome was provoked by pneumonia;
- impaired blood clotting and increased likelihood of blood clots, which can cause excessive hemorrhage;
- renal failure or complete failure of the functioning of this organ. In such cases, treatment will consist of lifelong dialysis or transplant surgery.
Untimely emergency care and improper therapy lead to the death of the patient within two days after the expression of the first symptoms.
Diet
Early initiation of nutritional support is recommended (in the first 24–36 hours), which is based on the following recommendations:
- The energy value of the diet is based on 25–30 kcal/kg body weight/day.
- Protein component: 1.3–2.0 g/kg/day.
- Lipids: 15–20% non-protein calories.
- Glucose: 50–60% non-protein calories, maintaining glycemic levels no higher than 6.1 mmol/L.
After relief of ITS, nutrition according to the recommendations for a specific infectious disease or Table No. 15 .
Prevention
To prevent infectious-toxic shock, it is recommended:
- Timely and adequate treatment of infectious diseases, especially accompanied by high bacteremia and high alertness to the possibility of developing ITS in patients with salmonellosis , lobar pneumonia , hypertoxic form of diphtheria , shigellosis , sepsis , meningococcemia , Legionnaires' disease , out-of-hospital abortions, complicated childbirth, purulent diseases, bacterial obstructive urinary tract diseases.
- Timely treatment of bruises and wounds with violation of the integrity of the skin with antiseptic drugs.
To prevent toxic shock syndrome from tampons, it is recommended for women to:
- alternate hygiene products (pads and tampons) every menstrual cycle, and if necessary - during one menstrual cycle (tampons during the day, and pads at night);
- carefully select tampons whose adsorbing capabilities correspond to the volume of discharge;
- change tampons every four hours, even if it is not yet completely saturated with discharge;
- Avoid using mechanical means of preventing pregnancy (intravaginal contraceptives - diaphragms/caps).
Etiology
The reasons for the progression of this condition are the combination of an acute infectious process and weakened human immunity. This syndrome is a common complication of the following diseases:
- typhoid fever;
- salmonellosis;
- pneumonia (of any nature);
- chicken pox;
- dysentery;
- meningococcal infection;
- influenza and ARVI.
Other nonspecific factors in the development of infectious-toxic shock in children and adults are:
- surgical intervention;
- any violation of the integrity of the skin;
- pathological labor activity;
- complicated abortion;
- allergic reactions;
- HIV or AIDS;
- substance abuse.
Another reason for this condition is the use of sanitary tampons by female representatives. This is due to the fact that when using such an item during menstruation, Staphylococcus aureus can enter the female body, which produces dangerous toxins. The disease often affects girls and women aged fifteen to thirty years. The mortality rate in this case is sixteen percent. In addition, there have been recorded cases of the occurrence of such a disorder due to the use of vaginal contraceptives.
The pathogenesis of infectious-toxic shock is the entry of a large amount of toxic substances into the circulatory system. This process entails the release of biologically active substances, which leads to disruption of blood circulation.