Meronem®
An antibiotic from the carbapenem group for parenteral use, resistant to human dehydropeptidase-1 (DHP-1), does not require additional administration of a DHP-1 inhibitor.
Meropenem has a bactericidal effect due to its effect on the synthesis of the bacterial cell wall. The potent bactericidal effect of meropenem against a wide range of aerobic and anaerobic bacteria is explained by its high ability to penetrate the bacterial cell wall, its high level of stability towards most β-lactamases and its significant affinity for penicillin binding proteins (PBPs). Minimum bactericidal concentrations (MBCs) are usually the same as minimum inhibitory concentrations (MICs). For 76% of the bacterial species tested, the MBC/MIC ratio was 2 or less.
Meropenem is stable in pathogen susceptibility tests. In vitro tests show that meropenem acts synergistically with various antibiotics. Meropenem has been shown in vitro and in vivo to have a post-antibiotic effect.
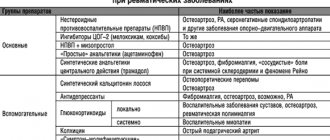
The only recommended criteria for sensitivity to meropenem are based on the pharmacokinetics of the drug and on the correlation of clinical and microbiological data - zone diameter and MIC determined for the relevant pathogens.
| Evaluation method | ||
| Pathogen category | Zone Diameter (mm) | MIC (mg/ml) |
| Sensitive | ≥ 14 | ≤ 4 |
| Intermediate | from 12 to 13 | 8 |
| Resistant | ≤ 11 | ≥ 16 |
The spectrum of antibacterial activity of meropenem, determined in vitro, includes almost all clinically significant gram-positive and gram-negative aerobic and anaerobic microorganisms.
The drug is active against aerobic gram-positive bacteria:
Bacillus spp., Corynebacterium diphtheriae, Enterococcus liquifaciens, Enterococcus avium, Listeria monocytogenes, Lactobacillus spp., Nocardia asteroides, Staphylococcus aureus (strains producing and not producing penicillinase), coagulase-negative staphylococci, incl.
Staphylococcus saprophyticus, Staphylococcus capitis, Staphylococcus cohnii, Staphylococcus xylosus, Staphylococcus warneri, Staphylococcus hominis, Staphylococcus simulans, Staphylococcus intermedius, Staphylococcus sciuri, Staphylococcus lugdenensis, Streptococcus pneumoniae (penicillin sensitive and resistant), Streptococcus agalact iae, Streptococcus pyogenes, Streptococcus equi, Streptococcus bovis, Streptococcus mitis, Streptococcus mitior, Streptococcus milleri, Streptococcus sanguis, Streptococcus viridans, Streptococcus salivarius, Streptococcus morbillorum, group G streptococci, group F, Rhodococcus equi; aerobic gram-negative bacteria:
Achromobacter xylosoxidans, Acinetobacter anitratus, Acinetobacter lwoffii, Acinetobacter baumannii, Aeromonas hydrophila, Aeromonas sorbria, Aeromonas caviae, Alcaligenes faecalis, Bordetella bronchiseptica, Brucella melitensis, Campylobacter coli, Campylobacter jejuni, Citrobacter freundii, Citrobacter diver sus, Citrobacter koseri, Citrobacter amalonaticus, Enterobacter aerogenes, Enterobacter agglomerans, Enterobacter cloacae, Enterobacter sakazakii, Escherichia coli, Escherichia hermannii, Gardnerella vaginalis, Haemophilus influenzae (including β-lactamase-producing strains and ampicillin-resistant strains), Haemophilus parainfluenzae, Haemophilus ducreyi, Helicobacter pylori, Neisseria meningitidis, Neisseria gonorrhoeae (including strains that produce β-lactamases and are resistant to penicillin and spectinomycin), Hafnia alvei, Klebsiella pneumoniae, Klebsiella aerogenes, Klebsiella ozaenae, Klebsiella oxytoca, Moraxella catarrhalis, Morganella morgannii, Proteus mirabilis, Proteus vulgaris, Proteus penneri, Providencia rettgeri, Providencia stuartii, Providencia alcalifaciens, Pasteurella multocida, Plesiomonas shigelloides, Pseudomonas aeruginosa, Pseudomonas putida, Pseudomonas alcaligenes, Pseudomonas cepacia, Pseudomonas fluorescens, Pseudomonas stutzeri, Pseudomonas pseudo mallei, Pseudomonas acidovorans, Salmonella spp., including Salmonella enteritidis, Salmonella typhi, Serratia marcescens, Serratia liquefaciens, Serratia rubidaea, Shigella sonnei, Shigella flexneri, Shigella boydii, Shigella dysenteriae, Vibrio cholerae, Vibrio parahaemolyticus, Vibrio vulnificus, Yersinia enterocolitica;
anaerobic bacteria:
Actinomyces odontolyticus, Actinomyces meyeri, Bacteroides-Prevotella-Porphyromonas spp., Bacteroides fragilis, Bacteroides vulgatus, Bacteroides variabilis, Bacteroides pneumosintes, Bacteroides coagulans, Bacteroides uniformis, Bacteroides distasonis, Bacteroides ova tus, Bacteroides thetaiotaomicron, Bacteroides eggerthii, Bacteroides capsillosis, Prevotella buccalis, Prevotella corporis, Bacteroides gracilis, Prevotella melaninogenica, Prevotella intermedia, Prevotella bivia, Prevotella splanchnicus, Prevotella oralis, Prevotella disiens, Prevotella rumenicola, Prevotella ureolyticus, Prevotella oris, Prevotella buccae, Prevotella denticola , Prevotella levii, Porphyromonas asaccharolyticus, Bifidobacterium spp ., Bilophilia wadsworthia, Clostridium perfringens, Clostridium bifermentans, Clostridium ramosum, Clostridium sporogenes, Clostridium cadaveris, Clostridium sordellii, Clostridium butyricum, Clostridium clostridiiformis, Clostridium innocuum, Clostridium subterminale, Clostridium tertium, Eubacterium lentum, Eubacterium aerofaciens, Fusobacterium mortiferum, Fusobacterium necrophorum, Fusobacterium nucleatum, Fusobacterium varium, Mobiluncus curtisii, Mobiluncus mulieris, Peptostreptococcus anaerobius, Peptostreptococcus micros, Peptostreptococcus saccharolyticus, Peptococcus saccharolyticus, Peptococcus asaccharolyticus, Peptostreptococcus magnus, Peptostreptococcus prevot ii, Propionibacterium acnes, Propionibacterium avidium, Propionibacterium granulosum.
Resistant to the drug
Stenotrophomonas maltophilia, Enterococcus faecium and methicillin-resistant staphylococci.
Meronem has shown effectiveness as monotherapy or in combination with other antimicrobial agents in the treatment of polymicrobial infections.
Meropenem (Meronem) in modern surgical practice
Despite the improvement of antibacterial therapy (ABT) and infection control measures, the problem of infectious diseases in surgical practice remains relevant to the present day. Particular challenges are associated with the treatment of severe and widespread infections caused by resistant microflora, which include complicated skin and soft tissue infections (SSTIs), including surgical site infections (SSIs), as well as intra-abdominal infections (IAIs) and abdominal sepsis. According to the US Centers for Disease Control and Prevention's National Nosocomial Infection Surveillance System (NNIS CDC), SSIs are the second most common (20%) and third most costly of all nosocomial infections and account for 38–40% of infections in surgical patients [1] . The development of SSI prolongs hospitalization by an average of 7–10 days and increases the relative risk of death by 2.2 times [2]. IAIs are life-threatening conditions and are the main reason for urgent hospitalization in surgical hospitals. Acute inflammatory destructive diseases of the abdominal organs are often complicated by the development of secondary peritonitis, the mortality rate of which ranges from 6.2 to 42.2% [3], and abdominal sepsis. It has been shown that the absence and delayed initiation of adequate ABT in IAI are accompanied by an increase in the incidence of severe complications, relaparotomies and mortality [4]. The severity of the course and the potential threat to the lives of patients determine the need for urgent initiation of effective ABT both in SSTI and in IAI. According to modern recommendations, initial antibiotic therapy for these infections should be carried out with drugs that are highly active against all probable pathogens, in optimal doses to ensure maximum effectiveness, minimal toxicity and reduce the risk of resistance selection [5]. Due to the wide spectrum of activity characteristic of all β-lactams, low toxicity, pharmacodynamics and pharmacokinetics, meropenem is one of the drugs of choice in the treatment of severe surgical infections. Mechanism of action and spectrum of antibacterial activity of meropenem The bactericidal effect of meropenem is realized as a result of the drug binding to penicillin-binding proteins, which leads to blocking the synthesis of peptidoglycan in the bacterial cell wall. Meropenem has a wide spectrum of action against gram-positive and gram-negative flora, as well as anaerobic bacteria. Although its activity is generally comparable to that of imipenem, it should be noted that meropenem has 2–8 times higher in vitro activity against gram(–) bacteria [6]. The activity of meropenem against gram(–) bacteria producing extended-spectrum β-lactamases (ESBLs) (Escherichia coli, representatives of the families Klebsiella, Serratia, etc.), as well as β-lactamases of the AmpC class (representatives of the Enterobacter and etc.). At the same time, a number of microorganisms, such as methicillin-resistant Staphylococcus aureus (MRSA), Enterococcus faecium and Stenotrophomonas maltophilia, as well as “atypical” intracellular pathogens (legionella, chlamydia and mycoplasma) exhibit natural resistance to meropenem, which may cause the ineffectiveness of empirical therapy for caused them infections. Despite more than 15 years of experience in the clinical use of meropenem, the sensitivity of most microorganisms to it has not undergone significant changes (Table 1). According to the results of the American branch of the MYSTIC project, which monitored the antibiotic resistance of nosocomial pathogens for the period from 1999 to 2008, including a total of 27,289 isolates, meropenem remained highly active against methicillin-sensitive strains of staphylococcus (460 strains, 100%), Streptococcus pneumoniae ( 125 strains, 80.2%) and other streptococci (159 strains, 90–100%), as well as representatives of Enterobacteriaceae (1537 strains, 97.3%). The drug had slightly less activity against Pseudomonas aeruginosa (439 strains, 85.4%) and Acinetobacter spp. (127 strains, 45.7%) [9]. According to the domestic project "RESORT", cefoperazone/sulbactam, imipenem and meropenem showed the greatest activity against 459 tested nosocomial strains of Acinetobacter baumannii (2.2, 2.2 and 3.5% of resistant isolates, respectively), the least - cefoperazone, gentamicin and piperacillin (97.8, 89.1 and 91.7%, respectively). P. aeruginosa (1053 strains) was characterized by a high frequency of resistance to all antibiotics, with the exception of polymyxin B, to which 5.8% of strains were insensitive. Among other antibiotics, the highest activity was observed for imipenem, meropenem, piperacillin/tazobactam and amikacin (39, 41.4, 41.6 and 42.4% of non-susceptible strains, respectively) [10]. It is significant that due to differences in resistance mechanisms, not all P. aeruginosa strains are cross-resistant to imipenem and meropenem. Thus, of the 411 imipenem-resistant strains identified during the RESORT project, 81.3% were insensitive to meropenem. Of the 436 strains resistant to meropenem, 76.6% were insensitive to imipenem [10]. Thus, the identified resistance to imipenem is not an absolute predictor of the ineffectiveness of meropenem, which dictates the need to determine the sensitivity of Pseudomonas aeruginosa to both drugs. At the same time, as part of this study, for the first time in Russia, strains of P. aeruginosa were identified that have complete cross-resistance to imipenem and meropenem due to the production of metallo-β-lactamases [11]. From the 2nd half of the 90s of the twentieth century. Until now, there has been a constant increase in the frequency of isolation of microorganisms that produce ESBLs. The results of determining the sensitivity of nosocomial strains of enterobacteria - ESBL producers, isolated in intensive care units (ICU) of various hospitals in Russia, indicate the undoubted superiority of carbapenems. Thus, 100% of E. coli, Klebsiella spp. and Proteus mirabilis collected in 2002–2004 were susceptible to imipenem and meropenem [12]. The results of foreign studies also showed the high activity of carbapenems against K. pneumoniae and E. coli, however, in recent years in the USA and European countries, the emergence of K. pneumoniae strains that are resistant to carbapenems due to the production of carbapenemases has been noted [13]. Thus, the use of carbapenems has not yet led to a significant decrease in sensitivity to them in a wide range of infectious agents, with the exception of P. aeruginosa. The wide distribution of ESBLs, capable of hydrolyzing not only penicillins, but also cephalosporins of the latest generations, has an extremely adverse effect on the prognosis and complicates the choice of therapy. Thus, it has been reliably shown that mortality increases by 1.7 times, the duration of hospitalization by 1.6 times, and the cost of treatment by 3 times for infections caused by ESBL-producing enterobacteriaceae [14]. In such a situation, carbapenems remain virtually the only group of antibiotics that are quite effective. Moreover, it has been shown that changing the dosing regimens of meropenem allows one to achieve an increase in the effectiveness of therapy, as well as to obtain a positive therapeutic response even in infections caused by strains regarded as resistant to this antibiotic. Meropenem dosage regimens and rationale The dose of meropenem for an adult with normal renal function is 0.5–1 g every 8 hours, but may be increased to 2 g every 8 hours for meningitis and other severe infections. Unlike imipenem, rapid administration of meropenem is not accompanied by an increased risk of nausea and vomiting, which allows the drug to be administered as an infusion over 20–30 minutes. or bolus over 3–5 minutes. At the same time, the results of many studies show that in certain clinical situations, a slower administration of meropenem (in the form of a 3-hour or continuous infusion) may be preferable. The activity of meropenem, like all β-lactam antibiotics, is time-dependent, i.e. is determined not by the maximum concentration of the drug, but by the time during which its concentrations exceed the minimum inhibitory concentration (MIC) - %T>MIC - for a particular pathogen. Carbapenems have been shown to exhibit bacteriostatic activity if their concentrations exceed the MIC for at least 20% of the dosing interval and bactericidal activity when this indicator increases to 40% or more [15]. The simplest method for optimizing the pharmacodynamic parameters of meropenem is to increase the dose or frequency of administration. In a comparative study, similar results were obtained with the use of meropenem at a dose of 500 mg every 6 hours and 1000 mg every 8 hours: clinical efficacy of 78 and 82%, respectively (p>0.05) with a significantly lower course dose (13 and 18 g, respectively) p=0.012) [16]. One of the promising ways to optimize pharmacodynamic parameters is the use of the drug in the form of an extended infusion, which makes it possible to obtain comparable values of pharmacokinetic parameters when using a 2-fold lower dose of the drug. Thus, %T>MIC at MIC 4 and 1 mg/l was 47 and 71%, respectively, with a 3-hour infusion of 500 mg and 43 and 67% with a 30-minute infusion of 1 g of the drug [17]. Another study using the Monte Carlo simulation method showed that an infusion of 500 mg meropenem over 3 hours was almost as bactericidal as a 2 g infusion over 30 minutes. [18]. Moreover, for MIC up to 16 mg/l with a 3-hour infusion of 2 g of meropenem, the %T>MIC indicator was 48%, which indicates the possibility of effective action on strains regarded as resistant to meropenem [19]. In particular, it was shown that the number of non-viable bacterial cells of P. aeruginosa after a 3-hour infusion of meropenem at a dose of 2 g reached 96%, while after an infusion for 1 hour it was 86.6% [20]. Rationale for the possibility of using meropenem in the treatment of surgical infections Starting ABT of surgical infections is usually carried out empirically and should be based on data on the structure (Table 2) and antibiotic resistance of pathogens, preferably local ones. IAIs have a polymicrobial etiology involving a wide range of gram-negative and gram-positive anaerobic and aerobic microorganisms. The leading role is played by gram-negative pathogens, mainly enterobacteria (E. coli, Proteus spp., Klebsiella spp., etc.), P. aeruginosa, and non-spore-forming anaerobes (especially B. fragilis). The frequency of isolation of gram-positive bacteria is less than 30% [5]. The causative agents of complicated SSTIs are represented by a wide range of microorganisms, the frequency of which depends on a number of factors, such as the place of origin and nature of the infection, its localization, etc. Gram-positive cocci are the predominant pathogens of community-acquired SSTIs, while gram-negative flora (E. coli, Enterobacter spp., Klebsiella spp., Proteus spp.) and P. aeruginosa are inherent in nosocomial processes. The likelihood of infection with P. aeruginosa increases when the lesion is localized in the lower extremities, the patient has severe somatic pathology, and also with SSI. Associations of microorganisms are often found [21]. The wide spectrum of activity of meropenem, including most pathogens of these infections, allows the use of this antibiotic as monotherapy, which reduces the risk of adverse interactions and increases the safety of treatment. A very important characteristic of meropenem for surgical practice is the ability to create therapeutic concentrations in the skin, exudate of skin elements, soft tissues, bile, pancreatic tissue, and peritoneal fluid [22,23]. Unlike a number of other drugs (cephalosporins, piperacillin/tazobactam), meropenem creates adequate plasma levels even in hemodynamically compromised patients in critical condition [24]. The results of the work of EJ Giamarellos–Bourboulis et al. are of no small importance. [25], according to which the use of meropenem is not accompanied by an increased risk of developing systemic endotoxicosis due to the lack of influence of the drug on the kinetics of endotoxins (bacterial lipopolysaccharides), C-reactive protein and interleukin-6 in patients with sepsis. A number of in vitro and animal studies have also shown that meropenem is significantly less likely to release exotoxins from P. aeruginosa, E. coli, Serratia marcescens and K. pneumoniae compared to other classes of antibiotics (including cephalosporins and fluoroquinolones). ) [7]. In addition, meropenem, along with imipenem, and unlike most other β-lactams, has a post-antibiotic effect against not only gram-positive, but also gram-negative bacteria. Thus, a slowdown in reproduction of varying degrees of severity was noted for S. aureus, P. aeruginosa, B. fragilis and E. faecalis and a number of other microorganisms [7]. Experience with the use of meropenem in the treatment of surgical infections The results of prospective clinical studies of the comparative effectiveness of meropenem and imipenem in the treatment of complicated SSTIs, presented in Table 3, demonstrate a high clinical (86.2–100%) and microbiological (88.5–94%) response to therapy meropenem. It should be noted that the lower efficacy rates in the study by TC Fabian et al. [28] are associated not so much with the increase in resistance of SSTI pathogens to carbapenems, but with the more severe nature of SSTI in the included patients. In particular, up to 80% of infections in both groups were deep, 18% were SSIs or secondary infected post-traumatic wounds. It is very significant that in the subgroup of patients with diabetes mellitus, the clinical effectiveness of meropenem was significantly superior to that of imipenem (86 and 72%, respectively, p < 0.0001), in contrast to patients without diabetes mellitus, in whom no differences were noted (87 and 89% respectively, p=0.322). In a systematic analysis of 79 randomized clinical trials of the ABT IAI, meropenem demonstrated high clinical efficacy (89%), comparable to that of piperacillin/tazobactam (90%) and aztreonam plus clindamycin (89%). Imipenem and other comparators had slightly lower efficacy (85% for imipenem, 87% for the combination of cefotaxime with metronidazole and ampicillin/sulbactam, 83% for the combination of tobramycin and clindamycin, and 80% for the combination of gentamicin and clindamycin). The authors of the review concluded that the effectiveness of monotherapy with any of the carbapenems is comparable to that for combination therapy, and the choice of antibiotic for a particular patient should be determined by the etiology of the disease and local data on the sensitivity of pathogens [29]. A systematic review of studies of the comparative effectiveness of meropenem and imipenem in the treatment of severe infections, including IAI, found no differences in the incidence of death (OR 0.98; 95% CI 0.71–1.35) in the comparison groups, however clinical (OR 1.04; 95% CI 1.01–1.06) and bacteriological efficacy (OR 1.05; 95% CI 1.01–1.08) were higher with meropenem treatment. In addition, meropenem demonstrated a better safety profile (OR 0.87 for adverse events; 95% CI 0.77–0.97) [30]. Another study showed equally high clinical and microbiological efficacy of carbapenems in the treatment of IAI (pathogen eradication rate: 98% in the meropenem group and 96% in the imipenem group; clinical effectiveness: 95 and 98%, respectively) [31]. The results of other comparative studies of the use of meropenem and imipenem also indicate their high effectiveness in the treatment of IAI (Table 4). The effectiveness of the use of meropenem and the new carbapenem drug doripenem in the treatment of IAI was comparable (clinical effectiveness - 85.3 and 85.9%, microbiological - 84.5 and 84.3%, respectively) [33]. In the course of a domestic prospective randomized study carried out in 2003–2004, a comparative assessment of the effectiveness of the use of meropenem and a combination of β-lactams and fluoroquinolones with aminoglycosides and/or metronidazole in the treatment of patients with severe nosocomial infection, including IAI with signs of sepsis, was carried out. According to the results obtained, meropenem was superior to standard therapy in terms of clinical effectiveness (recovery in 80.6 and 46.6% of patients in two groups, respectively, p<0.01) and the frequency of eradication of pathogens (89.6 and 48.1%, respectively, p< 0.01). When using meropenem, the probability of recovery from nosocomial infection was significantly higher (1.73–1.94; p <0.001) than in the control group. At the same time, the frequency of eradication of “problematic” pathogens was also higher in the meropenem group: P. aeruginosa (88% and 40%, respectively, p = 0.007), E. coli (100 and 46.7%, p = 0.003), Acinetobacter spp. (90.9 and 40%, p=0.02) [34]. Similar results were obtained in a previously conducted randomized trial by BI Kuo et al. The population of 53 patients demonstrated high clinical and bacteriological efficiency of meropenem in therapy of septic shock (clinical - 84% in the group of events and 76% in the Imipenem group, bacteriological - 80 and 75%, respectively) [35]. It must be emphasized that all of the above data was obtained during clinical studies using the original drug (Meronem, Astrazeneca UK Ltd.). As you know, not all generics have an equivalent quality, and the purpose of ineffective reproduced drugs leads to an additional risk of adverse outcomes of therapy and selection of resistant strains. In particular, according to the results of prospective clinical studies of therapy, 114 patients with nosocomial infections caused by A. Baumannii, and 199 patients with nosocomial infections caused by P. Aeruginosa, the use of generic forms of meropenem was a risk factor [36,37]. A comparative study of the properties of the original preparation of meropenem and generics showed that in the absence of differences in the indicators of the MPC and other pharmacokinetic parameters, they were not therapeutically equivalent [38]. Recently, the results of a comparison of the quality of Monem and one of the generations presented on the domestic market were published. Although the drugs did not have significant differences in the content and stability of the active component, as well as the spectrum and composition of water -soluble impurities, the investigated samples of the generic drug were characterized by unacceptably the long dissolution of the dissolution of the lyophilized contents in water (from 20 minutes to ≥3 hours) and contained a different number of insoluble particles . The previously conducted studies clearly demonstrate that the presence of insoluble particles detected in generics leads to a violation of microcirculation in ischemic tissues [39] can adversely affect the effectiveness of therapy and increase the risk of death, especially in patients with sepsis, septic shock and massive surgical surgical surgical. interventions [40]. The conclusion thus, the fast and adequate empirical antimicrobial therapy of surgical infections today can be ensured by the use of a wide range of effects of a wide spectrum of action, including potential pathogens of infection, including polyuretic gram -negative flora (producers of BLRS). The drugs of choice in such clinical situations are carbapenems, and the higher activity of meropenem in relation to gram -negative microorganisms, the features of pharmacodynamics and pharmacokinetics, as well as a favorable security profile make its use preferable. In the vast majority of studies in patients with severe and moderate infections of IAI and IKMT by the meropenem, but often exceeded comparison drugs prescribed both in the form of monotherapy and in the form of combinations. All of the above allows us to recommend meropenem for empirical monotherapy of patients with complicated IAI and IKMT in surgical hospitals, as well as in ith.
References 1. The Hospital Infection Control Practices Advisory Committee. Guideline for prevention of surgical site infection, 1999. Infect. Control. Hosp. Epidemiol. 1999; 20(4): 247–278. 2. Kirkland KB, Briggs JP, Trivette SL The impact of surgical–site infections in the 1990s: attributable mortality, excess length of hospitalization, and extra costs. Infect. Control. Hosp. Epidemiol. 1999; 20(11): 725–30. 3. Savelyev V.S., Gelfand B.R. Filimonov M.N. Peritonitis. Practical guide. M., 2006. 4. Falagas M.E., Barefoot L., Griffith J., et al. Risk factors leading to clinical failure in the treatment of intra–abdominal or skin/soft tissue infections. Eur J Clin Microbiol Infect Dis 1996; 15(12):913–21. 5. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated intra–abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Surg Infect (Larchmt) 2010;11(1):79–109. 6. Trouillet JL, Chastre J, Vuagnat A, et al. Ventilator–associated pneumonia caused by potentially drug–resistant bacteria. Am J Respir Crit Care Med 1998; 157(2): 531–539. 7. Hurst M., Lamb HM Meropenem: a review of its use in patients in intensive care. Drugs 2000; 59(3): 653–680. 8. Brown SD, Traczewski MM Comparative in vitro antimicrobial activity of a new carbapenem, doripenem: tentative disc diffusion criteria and quality control. J. Antimicrob. Chemother. 2005; 55(6): 944–949. 9. Rhomberg PR, Jones RN Summary trends for the Meropenem Yearly Susceptibility Test Information Collection Program: a 10–year experience in the United States (1999–2008). Diagn Microbiol Infect Dis. 2009; 65(4):414–26. 10. Reshedko G.K., Ryabkova E.L., Farashchuk A.N., Strachunsky L.S., ROSNET research group. Non-fermenting gram-negative pathogens of nosocomial infections in Russian ICUs: problems of antibiotic resistance. Klin Microbiol Antimicrob Chemoter 2006; 8:232–48. 11. Reshedko G.K., Ryabkova E.L., Krechikova O.I. et al. Antibiotic resistance of gram-negative pathogens of nosocomial infections in ICUs of multidisciplinary hospitals in Russia. Klin Microbiol Antimicrob Chemoter 2008; 10: 96–112. 12. Eidelshtein M.V., Strachunsky L.S. Dynamics of prevalence and sensitivity of ESBL-producing strains of Enterobacteriaceae to various antimicrobial drugs in Russian ICUs. Clin Microbiol Antimicrob Chemoter 2005;7:323–36. 13. Naas T., Nordmann P., Vedel G., et al. Plasmid-mediated carbapenem-hydrolyzing beta-lactamase KPC in a Klebsiella pneumoniae isolate from France. Antimicrob Agents Chemother. 2005;49(10):4423–4. 14. Lautenbach E, Patel JB, Bilker WB, et al. Extended–spectrum beta–lactamase–producing Escherichia coli and Klebsiella pneumoniae: risk factors for infection and impact of resistance on outcomes. Clin Infect Dis 2001;32(8):1162–71. 15. Mattoes HM, Kuti JL, Drusano GL, et al. Optimizing antimicrobial pharmacodynamics: dosage strategies for meropenem. Clin Ther. 2004; 26(8): 1187–98. 16. Kotapati S., Nicolau D., Nightingale C., et al. Clinical and economic benefits of a meropenem dosage strategy based on pharmacodynamic concepts in a large teaching hospital. Am J Health Syst Pharm 2004;61:1264–70. 17. Kuti JL, Dandekar PK, Nightingale CH, et al. Use of Monte Carlo simulation to design an optimized pharmacodynamic dosing strategy for meropenem. J Clin Pharmacol 2003;43:1116–23. 18. Drusano GL Carbapenem monotherapy, novel strategies to minimize ICU resistance. 41st ICAAC 2001. December 16. Special Report. 19. Drusano GL Prevention of resistance: a goal for dose selection for antimicrobial agents. Clin Infect Dis 2003;36(suppl. 1):42–50. 20. Drusano GL Strategies for maximizing power, minimising resistance. Clin Microbiol Infect 2001;7(Suppl 1):89. 21. Fish DN Meropenem in the treatment of complicated skin and soft tissue infections. Ther Clin Risk Manag. 2006;2(4):401–15. 22. Wiseman LR, Wagstaff AJ, Bergden RN et al. Meropenem. Review. Drugs 1995:50:73–101. 23. Soga Y., Ohge H., Ikawa K., et al. Peritoneal pharmacokinetics and pharmacodynamic target attainment of meropenem in patients undergoing abdominal surgery. J Chemother. 2010;22(2):98–102. 24. Taccone FS, Laterre PF, Dugernier T, et al. Insufficient β-lactam concentrations in the early phase of severe sepsis and septic shock. Crit Care 2010;14(4):R126. 25. Giamarellos–Bourboulis EJ, Mega A, Pavleas I, et al. Impact of carbapenem administration of systemic endotoxemia in patients with severe sepsis and Gram-negative bacteriemia. J Chemother 2006;18(5):502–6. 26. Lami JL, Wilson SE, Hopkins JA Adjunctive antimicrobials in surgery of soft tissue infections: evaluation of cephalosporins and carbapenems. Am Surg 1991;57:769–74. 27. Nichols RL, Smith JW, Geckler RW, et al. Meropenem versus imipenem/cilastatin in the treatment of hospitalized patients with skin and soft tissue infections. South Med J 1995;88:397–404. 28. Fabian TC, File TM Jr., Embil JM, et al. Meropenem versus imipenem–cilastatin for the treatment of hospitalized patients with complicated skin and skin structure infections: results of a multicenter, randomized, double–blind comparative study. Surg Infect 2005;6:269–82. 29. Holzheimer RG, Dralle H. Antibiotic therapy in intra-abdominal infections—a review on randomized clinical trials. Eur J Med Res 2001;6(7):277–91. 30. Edwards SJ, Emmas CE, Campbell HE Systematic review comparing meropenem with imipenem plus cilastatin in the treatment of severe infections. Curr Med Res Opin 2005;21(5):785–94. 31. Basoli A., Meli EZ, Mazzocchi P., Speranza V. Imipenem/cilastatin (1.5 g daily) versus meropenem (3.0 g daily) in patients with intra–abdominal infections: results of a prospective, randomized, multicentre trial. Scand J Infect Dis 1997; 29:503–8. 32. Bereznyakov I. G. Clinical use of carbapenems: when, which one, for how long? Clin Microbiol Antimicrob Chemoter 2006;4:325–49. 33. Lucasti C., Jasovich A., Umeh O., et al. Efficacy and tolerance of IV doripenem versus meropenem in adults with complicated intra–abdominal infection: a phase III, prospective, multicenter, randomized, double–blind, noninferiority study. Clin Ther 2008;30(5):868–83. 34. Yakovlev S.V., Beloborodov V.B., Sidorenko S.V. Analysis of the adequacy of starting empirical antibacterial therapy regimens for severe nosocomial infections (ASET study). Clin Pharmacol Ter 2006; 15(2). 35. Kuo BI, Fung CP, Liu CY Meropenem versus imipenem/cilastatin in the treatment of sepsis in Chinese patients. Zhonghua Yi Xue Za Zhi (Taipei) 2000;63(5):361–7. 36. Torres JA, Tafur JD, Briceno DF, Viollegas MV Generic Antibiotics are a Risk Factor for Mortality in Acinetobacter baumannii Infections in Colombian Intensive Care Units (ICUs). 49th ICAAC, San Francisco, California, USA, September 12–15, 2009. Poster# K–312. 37. Ruiz SJ, Briceno DF, Pacheco R, et al. Antimicrobial Therapy with Generic Meropenem (T/GM) is a Risk Factor for Mortality In ICU–acquired Infections by P. aeruginosa (IIPa) in Colombia. 50th ICAAC, Boston, USA, September 12–15, 2010. Poster# K327. 38. Agudelo M., Morales M., Cardeno J., Franco S., et al. Differences in Therapeutic Efficacy of a Generic Product (GP) of Meropenem (MER) Compared with the Innovator (INN) in Murine and Cavian Models of Human Infection. 49th ICAAC, San Francisco, California, USA, September 12–15, 2009. Poster# A1–020. 39. Lehr HA, Brunner J, Rangoonwala R, et al. Particulate matter contamination of intravenous antibiotics aggravates loss of functional capillary density in postischemic striated muscle. Am J Respir Crit Care Med 2002;165(4):514–20. 40. Nikulin A.A., Tsyuman Yu.P., Martinovich A.A., et al. On the question of the interchangeability of intravenous forms of original and generic drugs: are comparative studies needed? Clin Microbiol Antimicrob Chemoter 2010;12(1):31–40.
Meronem
Antibiotic from the carbapenem group for parenteral use. Resistant to dehydropeptidase-1, bactericidal (inhibits the synthesis of the bacterial cell wall), easily penetrates the bacterial cell wall, resistant to most beta-lactamases, has a high affinity for penicillin-binding proteins (PBPs). Bactericidal and bacteriostatic concentrations are practically the same. Among the known beta-lactam antibiotics, it has the highest activity against most aerobic and anaerobic gram-positive and gram-negative microorganisms.
Meropenem interacts with receptors - specific penicillin-binding proteins on the surface of the cytoplasmic membrane, inhibits the synthesis of the peptidoglycan layer of the cell wall (due to structural similarity), inhibits transpeptidase, promotes the release of autolytic enzymes of the cell wall, which ultimately causes its damage and death of bacteria.
Active against gram-positive aerobes: Bacillus spp., Corynebacterium diphtheriae, Enterococcus liquifaciens, Enterococcus avium, Listeria monocytogenes, Lactobacillus spp., Nocardia asteroides, Staphylococcus aureus (including penicillinase-producing), Staphylococcus spp. (coagulase-negative), incl. Staphylococcus saprophyticus, Staphylococcus capitis, Streptococcus pneumoniae (including penicillin-resistant), Streptococcus agalactiae, Streptococcus pyogenes, Streptococcus equi, Streptococcus bovis, Streptococcus mitis, Streptococcus viridans, Streptococcus salivarius, Streptococcus morbillorum, Streptococcus spp. (groups G and F), Rhodococcus equi;
gram-negative aerobes: Achromobacter xylosoxidans, Acinetobacter anitratus, Acinetobacter Iwoffii, Acinetobacter baumannii, Aeromonas hydrophila, Aeromonas sorbria, Aeromonas caviae, Alcaligenes faecalis, Bordetella bronchiseptica, Brucella melitensis, Campylobacter coli, Campylobacter jejuni, Citrobacter freundii, Citrobacter divers us, Citrobacter amalonaticus, Enterobacter aerogenes , Enterobacter agglomerans, Enterobacter cloacae, Escherichia coli, Gardnerella vaginalis, Haemophilus influenzae (including beta-lactamase-producing and ampicillin-resistant strains), Haemophilus parainfluenzae, Haemophilus ducreyi, Helicobacter pylori, Neisseria meningitidis, Neisseria gonorrhoeae (including beta-lactamase-positive strains, resistant s to penicillins and spectinomycin), Hafnia alvei, Klebsiella pneumoniae, Klebsiella aerogenes, Klebsiella ozaenae, Klebsiella oxytoca, Moraxella catarrhalis, Morganella morganii, Proteus mirabilis, Proteus vulgaris, Providencia rettgeri, Providencia stuartii, Providencia alcalifaciens, Pasteurella multocida, Pseudomonas shigelloides, Pseudomonas aeruginosa, Pseudomonas putida , Pseudomonas alcaligenes, Burkholderia cepacia, Pseudomonas fluorescens, Pseudomonas stutzeri, Stenotrophomonas. Salmonella spp., including Salmonella typhi, Serratia marcescens, Serratia liquifaciens, Serratia spp., Shigella sonnei, Shigella flexneri, Shigella dysenteria, Vibrio cholerae, Vibrio parahaemolyticus, Vibrio vulnificus, Yersinia enterocolitica;
anaerobic bacteria: Actinomyces israelii, Bacteroides spp. (including Bacteroides fragilis, Bacteroides vulgatus, Bacteroides variabilis, Bacteroides pneumosintes, Bacteroides coagulans, Bacteroides uniformis, Bacteroides distasonis, Bacteroides ovatus, Bacteroides thetaiotaomicron), Prevotella spp. (including Prevotella melaninogenica, Prevotella buccae, Prevotella denticola, Prevotella levii), Porphyromonas spp. (including Porphyromonas asaccharolyticus), Bifidobacterium spp., Clostridium perfringens, Clostridium difficile, Clostridium sporogenes, Clostridium cadaveris, Clostridium sordellii, Clostridium butyricum, Clostridium clostridiiformis, Clostridium tetani, Eubacter lentum, Eubacter aerofaciens, Fusobacterium mortifer um, Fusobacterium necrophorum, Mobiluncus curtisii, Mobiluncus mulieris, Peptostreptococcus anaerobius, Peptostreptococcus micros, Peptostreptococcus saccharolyticus, Peptococcus magnus, Peptococcus prevotii, Propionibacterium acne, Propionibacterium avidium, Propionibacterium granulosum.
Meronem, 1 g, powder for solution for intravenous administration, 10 pcs.
Adults
.
The dosage and duration of therapy should be based on the type and severity of the infection and the patient's condition.
The following daily doses are recommended:
500 mg IV every 8 hours for the treatment of pneumonia, urinary tract infections, gynecological infections such as endometritis, infections of the skin and skin structures;
1 g IV every 8 hours for the treatment of nosocomial pneumonia, peritonitis, suspected bacterial infection in patients with symptoms of neutropenia, as well as septicemia.
For the treatment of meningitis, the recommended dose is 2 g every 8 hours.
The safety of the 2 g dose as a bolus injection has not been sufficiently studied.
Dose in adult patients with impaired renal function
In patients with creatinine Cl less than 51 ml/min, the dose should be reduced as follows:
| Creatinine clearance, ml/min | Dose (based on unit doses of 500 mg, 1 g, 2 g) | Frequency of administration |
| 26–50 | one dose unit | every 12 hours |
| 10–25 | 0.5 dose unit | every 12 hours |
| <10 | 0.5 dose unit | every 24 hours |
Meropenem is eliminated by hemodialysis. If long-term treatment with Meronem® is required, it is recommended that a unit dose (based on the type and severity of infection) be administered at the end of the hemodialysis procedure to restore effective plasma concentrations.
Currently, there is no data on experience with the use of Meronem® for administration to patients undergoing peritoneal dialysis.
Dosing in Adult Patients with Hepatic Impairment
In patients with liver failure, there is no need for dose adjustment (see section "Special Instructions").
Elderly patients
In elderly patients with normal renal function or creatinine Cl more than 50 ml/min, no dose adjustment is required.
Children
For children aged 3 months to 12 years, the recommended dose for intravenous administration is 10–20 mg/kg every 8 hours, depending on the type and severity of the infection, the sensitivity of the pathogen and the patient's condition. In children weighing more than 50 kg, adult doses should be used.
For meningitis, the recommended dose is 40 mg/kg every 8 hours.
The safety of the 40 mg/kg bolus dose has not been sufficiently studied.
There is no experience in using the drug in children with impaired liver and kidney function.
Method of administration
Meronem® for IV use can be administered as an IV bolus injection over at least 5 minutes, or as an IV infusion over 15–30 minutes, using appropriate infusion fluids for dilution.
The possibility of using meropenem in an extended infusion mode (up to 3 hours) is based on pharmacokinetic and pharmacodynamic parameters. To date, clinical and safety data supporting this regimen are limited.
If a decision is made to treat a patient with an extended infusion method, then attention should be paid to the stability data of compatible infusion fluids (see table below).
Meronem® for IV bolus injections should be diluted with sterile water for injection (5 ml per 250 mg of meropenem), and the concentration of the solution is about 50 mg/ml. The resulting solution is a clear, colorless or light yellow liquid.
Meronem® for intravenous infusion can be diluted with a compatible infusion fluid (from 50 to 200 ml).
Meronem® should not be mixed with or added to other drugs.
Meronem® is compatible with the following infusion fluids:
0.9% sodium chloride solution;
5 or 10% dextrose solution;
5% dextrose solution with 0.02% sodium bicarbonate solution;
0.9% sodium chloride solution and 5% dextrose solution;
5% dextrose solution with 0.225% sodium chloride solution;
5% dextrose solution with 0.15% potassium chloride solution;
2.5 or 10% mannitol solution.
When diluting the drug Meronem®, standard asepsis should be observed. It is necessary to shake the diluted solution before administration.
All bottles are for single use only.
For IV injections and infusions, it is recommended to use a freshly prepared solution of Meronem®
Meronem®, reconstituted as described above, remains effective when stored at room temperature (below 25°C) or refrigerated (up to 4°C) for the times indicated in the following table:
| Solvent | Storage duration, h | |
| at 15–25 °C | at 4 °C | |
| A drug diluted with water for injection, intended for bolus injection | 8 | 24 |
| solutions (1–20 mg/ml) prepared using: | ||
| 0.9% sodium chloride | 8 | 48 |
| 5% dextrose | 3 | 14 |
| 5% dextrose and 0.225% sodium chloride | 3 | 14 |
| 5% dextrose and 0.9% sodium chloride | 3 | 14 |
| 5% dextrose and 0.15% potassium chloride | 3 | 14 |
| 2.5% dextrose or 10% mannitol for IV infusion | 3 | 14 |
| 10% dextrose | 2 | 8 |
| 5% dextrose and 0.02% sodium bicarbonate for intravenous infusion | 2 | 8 |
The Meronem® solution should not be frozen.