The cardia, or cardiac part of the stomach, is a cylindrical segment covering the esophagogastric junction and the space 2 cm above and below it. Cancer of the gastric cardia (cardioesophageal cancer, CER) differs in anatomical and clinical features, and requires a special approach to treatment. Many experts even identify it as a separate nosology, and there are several reasons for this:
- Tumors of this location tend to spread to the esophagus much more often than cancer of the underlying parts of the stomach.
- Such tumors metastasize to the abdominal and mediastinal lymph nodes.
- In addition, they have a poorer prognosis than gastric or esophageal cancer.
Cardioesophageal cancer is characterized by aggressive growth and a tendency to metastasize to the mediastinal lymph nodes.
- Causes
- Symptoms of gastric cardia cancer
- Classification
- Diagnostics
- Treatment of gastric cardia cancer
- Complications and relapses
- Prognosis and prevention
Causes
The causes of cardiac cancer are not reliably known. Currently, it is customary to talk about risk factors - circumstances under which the likelihood of developing a particular pathology increases. For stomach cancer they are as follows:
- Helicobacter pylori infection.
- The presence of atrophic gastritis of the proximal stomach.
- Hereditary predisposition.
- Smoking and alcohol abuse.
As for gastroesophageal reflux and Barrett's esophagus, these conditions are the main predisposing factors for the development of esophageal cancer, but they do not affect the incidence of cardia cancer.
How is food transported?
The structure of the stomach provides for the transportation of food coming from the esophagus and its simultaneous processing. The muscular layer of the wall includes 3 layers of smooth muscle:
- outside - longitudinal;
- in the middle - circular (circular);
- from the inside - oblique.
When muscle groups contract, the stomach acts like a “concrete mixer.” At the same time, rhythmic contractions occur in the segments, pendulum-like movements, and tonic contractions. Thanks to this, the food continues to be crushed, mixes well with gastric juice, and gradually moves to the pylorus.
The transition of a bolus of food from the stomach to the intestines is influenced by several factors:
- weight of content;
- maintaining the difference in pressure between the outlet of the stomach and the duodenal bulb;
- sufficiency of grinding of gastric contents;
- osmotic pressure of processed food composition (chemical composition);
- temperature and acidity.
Gastric juice ensures the “processing” of the food bolus
Peristalsis is enhanced by the vagus nerve and inhibited by sympathetic innervation. The fundus and body of the stomach ensure the deposition of food and the effect of proteolytic substances on it. The antrum is responsible for the evacuation process.
Symptoms of gastric cardia cancer
Cardia cancer is most characterized by weight loss, food aversion, pain and dysphagia. The pain is usually localized in the epigastric region, is constant, pressing in nature and does not depend on food intake. Sometimes it radiates to the lumbar region or behind the sternum. In the latter case, the disease can simulate heart pathology, such as angina.
The severity of dysphagia depends on the size of the tumor and obstruction of the digestive tract. It is mainly manifested by malnutrition, which leads to hypovolemia and changes in electrolyte balance.
Anatomical and physiological characteristics (APF) in children and the elderly
In the fourth week of pregnancy, the embryo begins to form the pharynx, esophagus, stomach and partially other digestive organs from the foregut. In newborns, the stomach is located horizontally. When the baby gets on his feet and begins to walk, the axis moves to a vertical position.
The volume of physiological capacity does not immediately correspond to the size of the organ:
- in a newborn it is only 7 ml;
- on the fifth day - 50 ml;
- for the tenth - 80 ml.
For a one-year-old child, a volume of 250 ml is considered normal. By three years it increases to 600 ml, by twelve - to 1.5 liters.
In the neonatal period, the cardia and fundus are the most poorly developed. The cardiac sphincter does not function sufficiently compared to the pyloric sphincter, so the baby often burps. There are still few secretory glands in the mucous membrane; functionally it is ready to receive only mother's milk. Gastric juice has the same composition as that of an adult, but its acidity and enzyme activity are much lower.
The baby's stomach produces the main enzymes:
- chymosin (rennet enzyme) - necessary for the digestion and curdling of milk;
- lipase - for the breakdown of fats, but it is still small.
Peristalsis of the muscle layer is slowed down. The time it takes for food to be evacuated into the intestines depends on the type of feeding: in artificial babies it is delayed for a longer period. The development of the total mass of the gastric glands is influenced by the transition to complementary feeding and further expansion of nutrition. By adolescence, the number of glands increases a thousand times. In old age, the position of the stomach returns to horizontal again, and prolapse often occurs.
Sizes are decreasing. The muscle layer gradually atrophies and loses tone. Therefore, peristalsis is sharply slowed down, food is delayed for a long time. At the same time, the cells of the mucous membrane become depleted and atrophy, and the number of secreting glands decreases. This is expressed in a decrease in the production of pepsin, mucus, and a decrease in acidity. In elderly people, due to a pronounced atherosclerotic process in the mesenteric arteries, the nutrition of the organ wall is impaired, which provokes the formation of ulcers.
Diagram of departments and their functional purpose
Classification
The classification of cardia cancer is based on the location of the center of the tumor. The anatomical reference point is the Z-line - the line of the esophagogastric junction.
- Type I cancer - the center of the tumor is located at a distance of 1-5 cm above the Z-line towards the esophagus.
- Type II cancer - the center of the tumor is located within 1 cm orally and 2 cm below the Z-line.
- Type III cancer - the center of the tumor is located at a distance of 2-5 cm below the Z-line.
Diagnostics
- Endoscopic examination of the stomach and esophagus. Allows you to examine the tumor and take a biopsy for morphological examination.
- Endoscopic ultrasound. It is carried out to determine the degree of tumor invasion, its growth into neighboring organs and structures, as well as to search for regional metastases.
- Abdominal ultrasound. It is carried out to search for metastases.
- X-ray contrast study. Allows you to determine the extent of the tumor and assess the degree of stenosis of the cardia and esophagus. The method is especially relevant for diffuse-infiltrative forms of cancer, when false-negative biopsy results can be obtained due to submucosal localization.
- CT scan is used to look for distant metastases.
- Diagnostic laparoscopy. Allows you to detect the spread of the tumor to the serous membranes, as well as diagnose intraperitoneal dissemination.
- Determination of tumor markers - CEA, CA 19-9, CA 72-4.
Neighboring organs
The anatomy of the human stomach is inextricably linked with the condition of neighboring organs. Therefore, it is important for a doctor to know the topography; we can call it a “3D vision” of connections with neighboring organs. The anterior surface of the stomach is partially adjacent to the diaphragm, the abdominal wall and the lower edge of the liver.
The posterior surface is in contact with the pancreas, aorta, spleen, the upper part of the left kidney with the adrenal gland, and partially with the transverse colon. The dense “neighborhood” is reinforced by nutrition from the same arterial branches, joint venous and lymphatic drainage. Therefore, the structure of the human stomach is subject to changes in pathological conditions of other internal organs.
We should not forget that behind the stomach around the superior mesenteric artery lies the solar plexus, which receives impulses from all the most important organs
Treatment of gastric cardia cancer
Treatment of cardia cancer requires a combined approach and includes chemotherapy and surgery. For unresectable tumors, the main treatment method is chemotherapy, and operations are performed for life-threatening indications.
Surgical treatment
The choice of the extent of the operation and surgical approach is determined based on the type of cancer and its local prevalence. For type I CER, proximal gastrectomy is performed
| KER type I Proximal gastrectomy, subtotal esophageal resection. | KER type II Gastrectomy (the entire stomach is removed), resection of the lower thoracic esophagus | KER type III Gastrectomy, resection of the lower thoracic esophagus. |
The minimum volume of lymph node dissection involves the removal of 1st and 2nd order lymph nodes (extended lymph node dissection is performed in the volume of D2). In CER I, bilateral mediastinal lymph node dissection is performed.
Chemotherapy
Chemotherapy is carried out using one of the following options:
- Perioperative chemotherapy. Performed in CF or ECF mode for 8-9 weeks before and after surgery.
- Adjuvant chemotherapy. It begins 4-6 weeks after surgery, if there are no severe complications, and is carried out for 6 months. XELOX or CAPOX schemes are used.
- Adjuvant chemoradiotherapy. Currently, it is rarely used and only in case of non-radical surgery.
Treatment of unresectable and disseminated tumors is carried out using chemotherapy according to the CF, CX, XELOX regimens in 6-8 three-week courses, or 9-12 two-week courses. After this, treatment is stopped and observation is carried out until the disease progresses. For HER2-positive gastric cancer, treatment with trastuzumab is possible.
After disease progression, chemotherapy is resumed, and the treatment regimen is selected taking into account the existing medical history.
Metastasis
With CER types I and II, metastasis mainly occurs in the lymphatic collectors of the paracardial zone, celiac trunk and lesser curvature of the stomach. In type I CER, the mediastinal nodes may also be involved in the process. Such features of metastasis are taken into account when planning surgery and lymph node dissection.
What cells provide the function of digesting food?
The structure of the mucous membrane is studied by histologists when diagnosing a pathological process. Normally it includes:
- cells of single-layer columnar epithelium;
- a layer called “intrinsic”, made of loose connective tissue;
- muscle plate.
The second layer contains its own glands, which have a tubular structure. They are divided into 3 subspecies:
- the main ones - produce pepsinogen and chymosin (digestive enzymes, in an acidic environment they turn into proteolytic enzymes);
- parietal (lining) - synthesize hydrochloric acid and gastromucoprotein;
- additional - form mucus.
Among the glands of the pyloric zone are G-cells that secrete the gastric hormonal substance gastrin. Accessory cells, in addition to mucus, synthesize a substance necessary for the absorption of vitamin B12 and hematopoiesis in the bone marrow (Castle factor). The entire surface of the mucosa in the deep layers contains cells that synthesize the precursor of serotonin.
The gastric glands are located in groups, so under a microscope, from the inside, the mucous membrane has a granular appearance with small pits and flat, irregularly shaped fields. The good adaptability of the healthy mucous membrane is noteworthy. It is capable of rapid recovery: the epithelium on the surface is replaced less than every 2 days, and the glandular one - in 2-3 days. A balance is maintained between old cells being rejected and newly formed ones.
In diseases of the stomach, hypertrophy of the glands, inflammation and cell death occur, dystrophic and atrophic disorders are accompanied by a failure in the production of necessary substances, scarring replaces the functioning tissue with non-functioning fibrocytes. Malignant cells transform into atypical ones. They begin to grow and release toxic substances that poison the body.
The secretory activity of the stomach is controlled by nervous and humoral mechanisms. The main influence on the functioning of the organ is exerted by the branches of the sympathetic and vagus nerves. Sensitivity is provided by the receptor apparatus of the wall and spinal nerves.
Complications and relapses
The main complications of cardioesophageal cancer:
- Tumor disintegration and bleeding. In this case, urgent endoscopic examination and bleeding control are required. If the problem cannot be solved endoscopically, surgical intervention is performed.
- Tumor stenosis. This complication leads to dysphagia and, as a consequence, to the development of nutritional disorders. To eliminate it, recanalization, balloon dilatation, and stenting are used. In severe cases, bypass anastomosis or gastrostomy removal is indicated.
- Pain. To reduce pain, radiation therapy, drug treatment and, in some cases, locoregional anesthesia are used.
- Ascites is an accumulation of fluid in the abdominal cavity. To eliminate it, diuretics and intracavitary chemotherapy are prescribed. When large volumes of fluid accumulate, laparocentesis is indicated - evacuation of the contents through puncture.
Prognosis and prevention
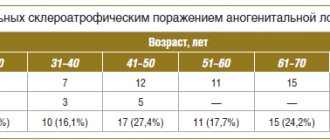
The 5-year survival rate for any type of CER averages 23.6%. Type III tumors have the most unfavorable course, since they are predominantly represented by poorly or undifferentiated neoplasms. The 5-year survival rate for this location is about 14%. The prognosis is significantly worsened by the presence of metastases in the mediastinal lymph nodes.
Euroonko employs doctors with extensive experience in treating stomach cancer. We are guided by current European standards. For this, the clinic has everything necessary - from the latest medications to modern equipment, thanks to which we are ready to provide assistance in the most severe cases.
Book a consultation 24 hours a day
+7+7+78