Tumor markers are specific substances found in the blood and urine, which can be both waste products of the tumor and substances synthesized by healthy cells in response to the invasion of cancer cells. Detection of tumor markers in the body makes it possible to diagnose the oncological process at an early stage and monitor the dynamics of pathology during treatment.
Who needs to be tested for tumor markers?
People whose relatives have been diagnosed with tumors of various locations should take tests for tumor biomarkers as screening tests 1–2 times a year.
People who have benign tumors (adenoma, myoma, fibroma) or tumor-like formations (kidney cysts, ovarian cysts) need to be examined with the same frequency. The rest can be tested for tumor markers once every 2-3 years.
People who have undergone cancer therapy should be tested for tumor biomarkers: every month during the first year, once every 2 months during the second year, once every 3 months during the third to fifth year. Five years after cancer treatment, it is sufficient to undergo tumor marker testing once every 6–12 months.
Tumor biomarkers can be detected in urine, blood, prostatic juice, fluid taken from the pleura or abdominal cavity. Specific antibodies are added to a sample of biological fluid taken from the patient. They form specific complexes with the protein structure of the tumor marker, which are identified by laboratory methods. Non-protein tumor biomarkers are determined by other methods.
Blood test for tumor markers at Family Doctor
When carrying out the analysis, the following indicators (tumor markers) are assessed first of all:
- AFP (alpha fetoprotein) is normally produced by the fetal membrane and is registered during pregnancy. In the absence of pregnancy, it indicates an oncological disease, primarily liver cancer;
- CEA (carcinoembryonic antigen) - indicates, first of all, rectal cancer; however, it can be detected in cancer of the lungs, mammary glands, and in some cases - in cancer of the thyroid gland, liver, bladder, cervix, and pancreas. Therefore, this tumor marker is considered nonspecific (i.e., indicating the presence of a malignant tumor in the body without being tied to any specific organ);
- PSA (prostate-specific antigen) is a marker of prostate cancer. Men over the age of 35 are recommended to undergo a PSA test annually to detect the disease at an early stage;
- CA 19-9 – pancreatic cancer marker;
- CA 15-3 – breast cancer marker;
- CA 125 is a marker for ovarian cancer.
- SCC – squamous cell carcinoma marker;
- Pro-GRP is a marker for small cell lung cancer.
At Family Doctor you can take a blood test for tumor markers at any of the clinics, choosing the one that is located in the area of Moscow you need. You can take a blood test for tumor markers on any day (including on weekends).
Most frequently identified tumor markers
75% of cancer patients have elevated alpha-fetoprotein (AFP) levels. Most often it is elevated in liver cancer; also, its high level can indicate testicular and ovarian cancer (in 5% of cases).
The tumor marker beta-2-microglobulin indicates the development of lymphoma and multiple myeloma. Markers CA 27-29, CA 15-3 indicate possible breast cancer, CA 125 - ovarian cancer. Biomarkers LASA-P, CA 72-4 make one suspect the presence of ovarian cancer and gastrointestinal tumors. The CA 19-9 marker is detected in cancer of the pancreas.
Recommendations for preparation
In order to obtain high-probability data, doctors should adhere to the following rules:
- donate blood early in the morning, on an empty stomach;
- if blood is donated in the afternoon or evening, then it is not recommended to eat for at least five hours before blood sampling (note that some laboratories advise not to eat twelve hours before the test);
- a few days before donating blood, it is necessary to exclude fatty foods, citrus fruits, orange-colored vegetables and fruits;
- It is also recommended to avoid drinking alcohol, smoking, and not being sexually active for a few days;
- It is also necessary to refrain from heavy physical activity and not to succumb to stress.
Tumor marker monitoring
Monitoring the dynamics of tumor markers plays an important role in cancer therapy. This allows you to determine the effectiveness of treatment and timely adjust its regimen. For example, during chemotherapy and radiation therapy, it is possible to increase the level of markers, which does not indicate an exacerbation of the process, but rather lysis of the tumor. Together with other indicators, biomarkers make it possible to monitor the patient’s health status during therapy and at its end.
You can get tested for tumor markers at the Medical Genetics Center.
Tumor markers. general information
The term “tumor markers”, or tumor markers (TM), combines a wide range of different high-molecular substances produced by tumor cells. This may include fetal proteins, hormones, enzymes, antigenic determinants detected using monoclonal antibodies, fragments of immunoglobulin molecules, etc. OMs are formed inside or on the surface of tumor cells, or under the influence of the tumor they are induced in other cells. One way or another, OM enter the bloodstream and can be quantified in peripheral blood or other biological fluid (urine, cerebrospinal fluid, pleural fluid, cyst contents, ascites, etc.).
Currently, more than 200 OMs are known, but only a few of them are of interest for clinical practice. There is no uniform classification of OM. From a clinical point of view, it is convenient to subdivide them according to the location and histological structure of the tumor. Table 14 provides information on the use of the most significant OMs in practice.
OM are widely used in the clinic. In combination with other research methods, they provide real assistance in diagnosing a malignant neoplasm, assessing the prognosis of the course of the disease and the radicality of the operation, early detection of relapses, monitoring the effectiveness of therapy, as well as obtaining additional information.
Diagnosis of cancer. Ideally, OM should be produced only by malignant tumor cells, and therefore should not be present in healthy people or in individuals with benign pathologies. In fact, no tumor-specific marker has been found.
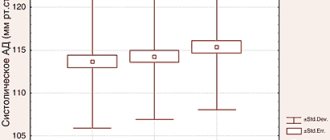
The diagnostic significance of OM is determined by three characteristics: diagnostic sensitivity, diagnostic specificity and discriminatory level or discriminatory concentration (DL, DC) (Fig. 7).
UL is the permissible upper limit of OM concentration in healthy people and in patients with benign diseases. All marker values that exceed the DL are considered positive or pathologically elevated.
Diagnostic specificity of OM is the frequency of true negative test results in a group of healthy individuals and/or individuals with benign pathologies, expressed as a percentage. Ideally, it should be 100% (Fig. 7, a), but in reality (Fig. 7, b) OM is always detected in a certain proportion of people who do not have cancer pathology, i.e. registration of false positive results. The lower the percentage of such results, the higher the specificity.
Diagnostic sensitivity of OM is the frequency of true positive test results in a group of cancer patients, expressed as a percentage. The higher the sensitivity, the less often false negative results are noted.
| Tumor localization | Histological structure of the tumor | Tumor markers |
| Liver | Hepatocellular carcinoma, hepatoblastoma | AFP |
| Cholangiocellular carcinoma | CA19.9 | |
| Colon and rectum | Adenocarcinoma | REA, SA19.9 |
| Anal canal | Squamous cell carcinoma | SCC, CYFRA21.1 |
| Stomach | Adenocarcinoma | CEA, CA19.9, CA72.4, pepsinogens I and II |
| Pancreas | Adenocarcinoma | CA19.9, CA242 |
| Esophagus | Squamous cell carcinoma | SSS, REA, CYFRA21.1 |
| Breast | Adenocarcinoma | SA15.3, REA |
| Ovary | Epithelial tumors | CA125, CA199, HE4 |
| Germ cell tumors | AFP+hCG | |
| Granulosa cell tumors | Inhibins | |
| Uterus | Adenocarcinoma | SA125, REA, HE4 |
| Choriocarcinoma | hCG | |
| Cervix | Squamous cell carcinoma | SCC, CYFRA21.1 |
| Testicle | Nonseminoma | AFP+hCG |
| Seminoma | LDH, HCG, NSE | |
| Thyroid | Medullary carcinoma | |
| Follicular, papillary carcinoma | Thyroglobulin, TSH, CEA | |
| Lung | Adenocarcinoma | REA |
| Squamous cell carcinoma | CYFRA21.1, SСС | |
| Small cell cancer | NSE, Pro-GRP | |
| Prostate | Adenocarcinoma | PSAtot., PSAfree/PSAtot. |
| Leather | Melanoma | S100 |
| Bladder and urinary tract | Squamous cell carcinoma; Transitional cell carcinoma | UBC, CYFRA21.1, TPS, TPA |
Sensitivity and specificity are not constant values. They can be changed in accordance with the assigned tasks. For example, if it is necessary to increase the detection of a corresponding pathology in a given group of people, the sensitivity of the marker should be increased. To do this, you need to reduce the remote control (move the remote control to the left in Fig. b). In this case, sensitivity will increase, but at the expense of specificity. On the contrary, if you need to increase specificity (reduce the proportion of false-positive OM values in the control group), you should increase the RL (shift the RL to the right in Fig. b). At the same time, specificity will increase, but at the expense of sensitivity, due to an increase in the number of “missed” cancer patients. Consequently, the sensitivity and specificity of OM are interrelated in such a way that an improvement in one of these characteristics is accompanied by a deterioration in the other. In practice, they always try to find a reasonable compromise and set the RL for OM such that the specificity is 95–98%. In this case, sensitivity can vary widely - from 15% to more than 90% for different OMs or for the same OM used in the diagnosis of different tumors.
The use of OM for diagnostic purposes is very limited. Due to insufficient sensitivity and specificity, most circulating OM are unsuitable for detecting cancer pathology in an asymptomatic population. And although the sensitivity of many markers exceeds 80%, this value applies in most cases to the late stages of the disease. In the early stages, when treatment may be effective, the sensitivity of most OMs does not reach 50%. However, in groups with an increased risk of a particular malignant neoplasm, as well as in patients with corresponding symptoms (i.e., in cases where the frequency of this disease significantly exceeds the general population), the use of OM makes it possible to early detect a number of tumors.
When using OM for diagnostic purposes, it should be taken into account that:
- OMs are never used to make a diagnosis on their own, but only as an addition to other diagnostic procedures and always taking into account clinical data;
- Only OMs with a sensitivity of at least 50% can have diagnostic value.
Assessment of disease prognosis.
When detecting a malignant neoplasm, predicting the course of the disease is an important clinical task. The use of various prognostic factors and calculation of prognosis bring real benefits in cancer treatment. They are of great interest not only for calculating survival rate, but also serve to divide patients into risk groups, according to which additional therapy (chemo-, hormonal or radiation) is prescribed to surgical treatment, designed to destroy tumor formations not detected during surgery, which can lead to to the appearance of metastases. For patients with good and poor prognosis of the disease, differentiated treatment regimens are used, which are tested in randomized trials. This can have a positive impact on the patient’s quality of life, tolerance to therapy, treatment effectiveness and rational savings. The levels of most OM before treatment correlate with the main prognostic factors - tumor size, lymph node involvement, the presence or absence of metastases, histological type and degree of tumor differentiation, etc. For many OMs, their significance as independent prognostic factors has been shown.
Assessment of the radicality of the operation.
After radical removal of the tumor, the concentration of OM in the blood should decrease in accordance with its half-life. T1/2 is the time required to reduce the OM concentration by half after radical tumor removal. T1/2 varies significantly among different OMs - from several hours for β-hCG to several days for CEA. These data may be important in assessing the effectiveness of treatment. If the rate of marker decline is significantly lower than theoretical, then with a high degree of probability the presence of hidden metastases can be assumed.
Monitoring during remission.
At the end of treatment, the patient must be under the supervision of an oncologist with mandatory regular determination of OM. With negative OM values, no relapse is observed. An increase in OM with a high degree of probability indicates a relapse, the clinical symptoms of which can be noticed only 3-6 months later. Therefore, in some cases, for example, with germ cell tumors, an increase in the level of OM is a sufficient basis for starting chemotherapy, which can improve long-term results.
Evaluation of treatment effectiveness. Numerous literature data indicate that tumor regression is accompanied by a decrease in the level of the corresponding marker in the blood serum to normal values. The absence of changes or an increase in OM values gives reason to think about the tumor’s resistance to the therapy and is the basis for revising its tactics.
When interpreting the results, one should take into account many factors that can influence the level of OM: hereditary, racial, gender, age, physiological state, circadian rhythms and daily changes, bad habits, diagnostic tests (non-invasive and invasive), the course of the postoperative period, benign pathologies, medications.
To determine OM, various immunochemical methods are used - RIA, ELISA, ICL, ECLA, etc. When interpreting the results, it is important to take into account the method by which OM was determined, and if it is necessary to dynamically determine OM over a long period of time, it is recommended to carry out analyzes in the same laboratory. This is important because immunological methods based on the use of monoclonal antibodies identify individual epitopes, the number of which on a single molecule can vary widely between individuals. The expression of epitopes can vary significantly depending on the physical conditions and structural features of the molecule. Many modern methods recognize epitopes cleaved from the molecule, as a result of which it is possible to obtain results that are difficult to compare from both a clinical and analytical point of view. When OM is routinely determined in different laboratories, differing results may be a function of the method used. For example, when determining hCG, anti-beta, anti-alpha and anti-beta/alpha antibodies can be used. In any case, it is necessary to consider the method and factors that may cause false-positive results.
The content of most OM is determined in the blood, some in the urine. To determine the conditions for taking and storing biosamples, you should follow the instructions for the reagent kit used.
Preparing for analysis
To diagnose cancer using a blood test, material is taken from a vein. In this case, the conditions for storing the serum before the study must be observed, and it must be carried out no later than an hour after collection.
If at the time of the analysis there are signs of inflammation, then you need to report this, as the test results may become false positive. It is better to carry it out a week after the process has subsided. The same applies to the period of menstruation.
You should not drink alcohol the day before the test.
Taking ascorbic acid, some hormonal drugs, nitrates and other medications can also affect the level of OM. The doctor will tell you how long before the test you should stop taking them.
It is better to take all subsequent tests in the same laboratory so that the dynamics can be assessed.
Where can I donate tumor markers?
To undergo such tests, it is better to choose specialized clinics. Therefore, it is advisable to consider medical institutions that have the necessary equipment and qualified specialists who are able to correctly interpret test results.
In this case, the patient will be able to get the correct diagnosis the first time, and he will not have to waste personal time on additional research. You can also get tested at regular municipal clinics. But practice shows that after these examinations, patients turn to specialized institutions for a retake.