This disease has a symptom such as swelling (edema). One of the most common causes of arm lymphostasis is surgery performed for oncological reasons, for example, removal of the mammary gland (mastectomy). During this procedure, resection (removal) of lymph nodes, which are areas of regional metastasis, is performed. The lymph flow slows down sharply, and pathology begins to develop. Radiation therapy used during oncology treatment “seals” the lymphatic vessels, further impairing the outflow of lymph.
Prices for treatment and doctor's appointments in our center
| Basic services | price, rub. |
| Consultation with a doctor, lymphology specialist | 3 000 |
| Consultation with the head physician | 4 000 |
| Chiropractor consultation | 3 000 |
| Price of decongestant therapy | from 2500 per procedure |
| Taking measurements for the production of compression hosiery | 2 000 |
| Compression jersey | >Price, rub. |
| Jobst Basic circular knit compression socks | 4 000 |
| Jobst Basic circular knit compression tights | 6 500 |
| Jobst Basic Circular Knit Compression Stockings | 6 100 |
| Bandage system for arm and leg | From 100 euros for 1 segment |
| Custom-made compression socks and flat knit socks | Without additional options from 90 euros |
| Massages | price, rub. |
| Manual lymphatic drainage | From 2500 per procedure |
Make an appointment
Exercises to prevent lymphostasis
Exercise therapy is performed from the first day after surgery. It includes breathing exercises and a simple load on the hand (clenching and unclenching the fist, flexing and extending the elbow joint). Then, from the second to the sixth day, exercises are added, performed on a chair with a fixed back and relaxed lower limbs:
- Stretch your neck as high as possible, with your chin turned inward. Then turn your head to the sides. The gaze is directed “over the shoulder.” Then bend to the right and left, so that the ears touch the shoulders. The latter are in a fixed position;
- as you inhale, simultaneously raise both shoulders up to your ears, the position is maintained for several seconds, then as you exhale, lower them down;
- pull your shoulders back, fix this position, then relax the muscles;
- back straight. Raise your shoulders up and move them as far back as possible with rotational movements, then lower them down;
- Slowly raise straight arms at the elbows up (to the level of the shoulder girdle or until painful sensations appear), while relaxed fingers form a lock.
From the seventh day onwards the complex expands significantly:
- Place your palms behind the back of your head, your elbows pointing in opposite directions. With each inhalation, press your elbows towards each other;
- hands alternately rest on opposite shoulders;
- both shoulders arch back, arms turn outward (shoulder blades join together), exhalation is delayed for several seconds. Then you need to exhale and relax your arms, placing them along your body;
- a strong rope is used (its length should be 3 times the length of your arm). Make a knot at one end for easy fixation. Tie the other end to the handle of the closed door. The woman moves away about 1.5 meters and begins to rotate the rope with the hand of the operated side. Ideally, the elbow should be straight;
- the ends of the rope are thrown over the open door, hanging freely. The woman takes them in her hands while sitting (the door is located between her knees). The forearm on the operated side is initially bent. The woman begins to alternately pull the rope in opposite directions (movements similar to the motion of a saw). The gaze is directed forward (in front of oneself);
- the woman stands straight with her back to the wall. The shoulder girdle is fixed. Straight arms smoothly rise up to shoulder level and higher (ideally above the head), then just as slowly fall down;
- a rope or stick is used. The woman holds it so that the distance between the hands exceeds the width of the body. Feet are shoulder-width apart. The stick is raised with outstretched arms forward and up above the head. Then it is wound behind the back of the head. Then the movements are performed in reverse order.
Classes are held daily, with a gradual increase in load and pace. Most exercises can be performed in a lying or sitting position. In the latter case, maintaining a strictly vertical body position is considered important.
In addition, proper deep breathing throughout the entire workout is of great importance. All movements must be performed carefully, without jerking. Each exercise is performed 10-15 times. If pain or discomfort occurs, stop the activity. If symptoms do not go away, a woman should definitely consult a doctor. [2], (pp. 16-19)
A program for the prevention of arm lymphostasis after mastectomy is always developed individually for each woman, taking into account the characteristics of her body and physical fitness. To avoid unpleasant consequences and complications, a qualified specialist must draw up a physical therapy program.
What is hand lymphostasis?
Lymphostasis of the hands is a serious disease.
Due to a violation of the outflow of lymph, excessive accumulation of intercellular fluid rich in protein occurs, resulting in swelling of the soft tissues of the upper limb. With lymphostasis, there is an increase in the volume of subcutaneous fat due to edema. In the absence of proper treatment, gradual sclerosis and tissue fibrosis occur. If you do not seek professional help from qualified specialists, the disease progresses: swelling increases, changes appear on the skin in the form of hyperkeratosis, papillomatosis, maceration and ulceration, and infection occurs (nail and skin fungus, erysipelas).
Treatment of lymphedema
Unfortunately, it is very difficult to completely cure lymphedema. However, there are treatments that can help reduce swelling and pain.
The anti-edematous therapy complex is a complex of therapeutic measures that consists of 4 components and has 2 phases of treatment. Therapy begins with an intensive phase of therapy, during which the patient receives daily treatment and education, which can last up to 6 weeks. Next comes the maintenance phase, when the patient independently does everything that the doctor recommended at home, naturally, with monthly monitoring.
Components of therapy:
- Manual and hardware lymphatic drainage massage (performing and teaching the patient massage techniques is carried out not just by a massage therapist, but by a specially trained lymphologist).
- Compression bandage (applying compression at several levels with long and short stretch bandages to improve lymph outflow and prevent stagnation, then switching to compression stockings-sleeves of class 2-3-4 depending on the severity of the disease).
- Corrective gymnastics (this is a set of light exercises aimed at improving lymphatic drainage, each patient receives his own individual training plan from the treating physiotherapist)
- Responsible skin care of the affected limb (proper and daily skin care reduces the risk of infection (cellulite), patients are taught to reduce the risk of cuts/abrasions, etc.)
History has shown that surgical treatments for lymphedema have had disappointing results. However, a new surgical method using liposuction has proven to be more successful than its predecessors. After removing fatty tissue from the affected limb, swelling noticeably decreases, but wearing compression garments after manipulation is mandatory for at least 1 year. This method is acceptable from a clinical safety point of view, but there is no adequate experience of its long-term effectiveness.
What are the possible complications of lymphedema?
- Skin infections.
- Cellulitis is a bacterial infection of the skin and subcutaneous tissues. These patients are at high risk of developing sepsis. Cellulite is treated with antibacterial drugs.
- Lymphangitis, erysipelas. This is an infection of the lymphatic vessels (usually streptococcal), usually accompanied by a pathological reaction of the immune system to the pathogen. Treatment with antibacterial and antihistamine drugs.
- Depression. The diagnosis of lymphedema radically changes the lives of patients: it is not only a daily struggle with the disease, but also reconciliation with innovations in a person’s life - constantly wearing compression, regardless of the weather, changing the appearance of the affected limb. It is quite difficult to survive a stressful situation on your own.
Don't be left alone with your problems. Visits with a psychotherapist are part of overall treatment.
What are the causes?
Identifying the onset of development of elephantiasis in the hands allows you to prescribe the most effective treatment. This mechanism can be triggered by various factors, which are often interrelated. Among the most common factors leading to the progression of arm lymphostasis are the following:
- surgery to remove lymph nodes;
- negative effects of radioactive radiation in the treatment of oncology;
- serious injuries accompanied by damage to lymph nodes and blood vessels;
- fractures with a violation of the integrity of bone tissue in the form of comminuted fractures;
- infectious diseases and pathological neoplasms in the lymphatic system.
Diagnostics
It is possible to establish a preliminary diagnosis already at the first examination of the patient and by studying the anamnesis. The specialist’s assumptions can be confirmed by:
- Ultrasound of the abdominal cavity and pelvis to clarify the condition of the kidneys and excretory system;
- Ultrasound of the veins of the upper extremities;
- Chest X-ray;
- Lymphography using an X-ray machine;
- Lymphoscintography;
- Computer or magnetic resonance imaging.
The conclusion about the stage and type of the disease is made based on the comprehensive results of all the listed examinations.
Introduction
Lymphedema of the lower extremities is a chronic disease characterized by progressive high-protein edema of the extremity as a result of decreased lymph transport [1].
Chronic lymphedema represents a serious medical and socioeconomic problem. Around 150 million people worldwide suffer from lymphedema [2]. According to official data from the World Health Organization, this figure is several times higher - about 700 million people. The social significance of the problem, in addition to its widespread prevalence, is due to the predominance (up to 90%) of working age patients among patients [3, 4]. The disease mainly affects young and middle-aged women [5]. In the general structure of vascular pathology, lymphedema of the lower extremities occupies about 10% [6, 7]. The progressive course of the disease has a significant impact on the quality of life and work ability of patients - from aesthetic problems in the early stages to persistent disability in decompensated forms.
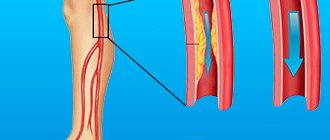
The lymphatic system of the lower extremities performs two main functions: 1) regulates the volume of tissue fluid and prevents the formation of edema; 2) removes proteins from tissues and returns them to the bloodstream. The occurrence of edema is associated with an imbalance between capillary filtration and lymphatic drainage [8].
Pathogenesis of lymphedema
Based on etiology, primary and secondary lymphedema are distinguished. The cause of the development of primary lymphedema is genetically determined defects of the lymphatic system [9].
Secondary lymphedema develops as a result of disruption or removal of lymphatic vessels and nodes, trauma, damage to the lymphatic tract during operations (phlebectomy, liposuction, arterial reconstruction) and inflammatory diseases (lymphadenitis, lymphangitis) [10].
Regardless of the etiology, the pathogenesis of lymphedema is based on insufficiency of the transport function of the lymphatic system, which leads to impaired outflow of lymph from tissues and a decrease in the resorption function of lymphatic capillaries [9, 11].
The initial stage of the disease is characterized by slight swelling that goes away after rest. As the disease progresses, edema becomes constant and tissue hypoxia increases. In later stages, the skin thickens due to the development of fibrosis and sclerosis, hyperkeratosis, papillomatosis, and lymphorrhea are formed [12].
Treatment of lymphedema of the lower extremities
Currently, there are two main directions in the treatment of lymphedema: conservative and surgical.
Surgical treatment of lymphedema can be divided into radical and reconstructive surgery.
According to international standards for the treatment of lymphedema, surgical intervention is offered to the patient only if long-term conservative therapy is ineffective [13], which is both a mandatory stage of preoperative preparation and the main type of treatment that improves the quality of life of patients.
The main goals of conservative treatment should be considered to reduce clinical manifestations and prevent relapses of the disease, prevent complications, and improve the quality of life of patients.
It is extremely important to create a system of education for patients themselves, aimed at changing lifestyle and preventing the progression of the disease, including [14]:
— lifestyle correction;
— avoid prolonged static loads;
- engage in active sports (running, cycling, race walking, swimming);
- during sleep and rest, place the lower limbs on a hill, at an angle of 5-10° to the body;
— exclude high-temperature effects (bath, sauna);
— nutrition correction: hypocaloric diet to control excess body weight and combat obesity;
— control over the condition of the skin of the lower extremities.
Pharmacological therapy includes the use of drugs with a polyvalent mechanism of action (detralex, troxerutin), which improve lymphatic and venous outflows, contractile activity of lymphatic vessels, and correction of inflammatory and trophic changes in tissues [15]. In addition to the lymphokinetic effect, troxerutin has the ability to split protein molecules into small fragments with a molecular weight of less than 10,000, which can penetrate into the venous bed through fenestrae of small venules and interendothelial connections of the venous part of the capillary bed [16]. Cleavage of long protein chains also facilitates phagocytosis of smaller fragments by macrophages [17]. Antimicrobial agents (long-acting antibiotics for up to 4-6 months) are prescribed for the treatment of erysipelas. In modern practice, semisynthetic penicillins, cephalosporins, macrolides, lincosamide group drugs, tetracyclines, vancomycin, minocycline, and fluoroquinolones are used in the treatment of erysipelas [18]. When a mycotic infection occurs, antifungal agents are used.
Conservative therapy for lymphedema includes compression treatment, therapeutic physical training, and the complex use of natural and preformed physical factors [3, 19].
Thanks to progress in the study of the pathogenesis of the disease and the development of new physiotherapeutic methods, in modern complex treatment of lymphedema, physiotherapeutic methods of influence are used pathogenetically justified [12].
Treatment of lymphedema should be aimed at reducing lymph formation, increasing the transport capacity of the lymphatic system, and improving venous outflow.
The following main directions of conservative treatment can be distinguished:
— limitation of lymph formation: elevation of the limb, elimination of exposure to high temperature, elastic compression [20];
— strengthening lymphatic drainage [21];
— stimulation of the contractile activity of lymphatic vessels (massage in an electrostatic field from the Khivamat apparatus, electrical stimulation with various types of currents);
— activation of contraction of muscle fibers of lymphatic vessels (amplipulse therapy, cryoamplipulse therapy, contrast baths, underwater shower massage);
- increased skeletal muscle tone;
— improvement of microcirculation (magnetic therapy, laser therapy, peloid therapy, thalassotherapy, balneotherapy, cryotherapy) due to changes in the tone of arterioles, capillaries and venules [22].
An important method of rehabilitation of patients with lymphedema of the lower extremities is therapeutic physical education. Elevation of the lower limb helps reduce the severity of edema. The basis of therapeutic exercises for patients with lymphedema are exercises aimed at turning on the muscular-venous pump of the lower extremities. The main goal of physical training is to increase the elasticity of the muscles and dermis in order to improve lymphatic and venous drainage [23].
In order to enhance the activity of lymphatic vessels, lymphatic massage is used. Massage movements are performed along the lymphatic pathways towards the nearest lymph nodes. The therapeutic effect of lymphatic massage is temporary, so it is necessary to conduct repeated courses 1-2 times a year [23].
In a study conducted by T.P. Shagivaleeva et al. in 2013, it was found that the integrated use of therapeutic physical culture and lymphatic massage increases therapeutic effectiveness, which is confirmed by the regression of edema syndrome [24].
The results of studies on the use of elastic compression, which is the basis for the treatment of limb lymphedema, without which no rehabilitation program can do, are widely presented in Russia and abroad. Compression treatment (use of medical knitwear or elastic bandages) is a pathogenetic, safe method of treatment. The therapeutic effect of elastic compression is due to an increase in the reabsorption of tissue fluid and proteins in the venous limb of the capillary and a decrease in its filtration in the arterial limb due to increased tissue pressure, resulting in regression of edema. As a rule, compression hosiery is made individually for each patient and has significant advantages compared to traditional bandaging: physiological distribution of pressure regardless of the skills of the patient or doctor, creation of favorable conditions for water and temperature balance of the skin of the limb, compliance with aesthetic requirements, the ability to choose the optimal pressure in accordance with the compression class of the product. The method is based on constant compression of the skin and subcutaneous tissue. Compression treatment helps prevent the progression of edema and reliably consolidate the effect of complex therapy [12].
In European practice, the principle of combined use of physical factors affecting various parts of the pathogenesis of lymphedema has become widespread. The most well-known clinical approach is a two-stage complex therapy method developed by M. Foldi, known as Complex Decongestive Therapy (CDT) [25]. Today, treatment of lymphedema abroad according to the principles of CDT is the official method of treating lymphedema. One of the main components of CDT is manual lymphatic drainage (MLD). MLD was originally developed by E. Vodder in 1936 as a cosmetic procedure. Subsequently, M. Foldi proved the high effectiveness of the method, thanks to which in the 70s MLD was accepted by insurance companies as a method of treating lymphedema. Nowadays, MLD is used according to the original methods of M. Foldi and E. Vodder [26].
Recently, the method of lymphatic aqua drainage has become widespread, aimed at activating the movement of the muscles that flex, extend and adduct the hip [27]. The advantage of this method is that the patient independently activates lymphatic drainage through physical exercises performed in a pool, where the resistance of the water acts as a massager, mechanically affecting the tissues [28, 29].
A number of authors have proposed the use of a gravity therapy unit in the complex rehabilitation treatment of patients with lymphedema of the lower extremities. The device is a horizontally located short-range electric centrifuge. The authors explain the positive effect by the redistribution of lymph, increased lymph drainage, and increased activity of preserved lymphangions, mainly in patients with stages I and II of the disease in response to gravitational influence [30].
Intermittent pneumatic compression procedures have high clinical and hemodynamic effectiveness [31, 32], which influence almost all parts of the pathogenesis of lower extremity lymphedema and contribute to the maximum reduction of the main clinical manifestation of this disease - edema [33-36].
Recently, a technique with alternating compression and MLD has become widely used. Compression reduces the formation of lymph, lowers hydrostatic pressure and tissue tension, and maintains the elasticity of the skin and subcutaneous tissue. With the help of massage, the function of reserve blood capillaries is stimulated, the surface of capillary filtration increases [37, 38].
Previously, methods of electromyostimulation with various types of currents were actively used (for example, amplipulse therapy - stimulation of the neuromuscular system with sinusoidal modulated currents). These methods were effective only in the initial stages of the disease, when the contractile functions of the lymphangion were not impaired [39]. The use of electromyostimulation improves lymphatic drainage due to collateral vessels and stimulation of the muscle-venous pump of the leg [40]. Various methods of cryotherapy (cryomassage and cryoampulse therapy) with temperatures of moderate cold (from 0 to –20 ° C) have proven their effectiveness in stages II and III of the disease. The method is based on the effects of “cold hyperemia” and “cold drainage”, which reduce spasm of arterioles and precapillaries, venous congestion in venules, pressure in the venous part of the capillary, lymph formation, and increase reabsorption [41].
It has been proven that low-intensity laser radiation stimulates lymphogenesis, restores lymphatic drainage by increasing the motility of lymphatic vessels and reducing the formation of interstitial fluid, having a beneficial effect on the endothelial function of blood vessels [42-45]. Additional effects of this method are reduction of fibrosis and sclerosis of lymphedema tissues due to the protective effects of fibroblasts, stimulation of immunity due to activation of macrophages [46, 47].
The combination of low-intensity laser therapy and a constant magnetic field (magnetic laser therapy) increases the penetrating ability of laser radiation, reduces its reflection at the tissue interface and improves absorption, which leads to an increase in the therapeutic effectiveness of laser therapy and the cumulation of the effects of both factors. With magnetic laser therapy, there is an improvement in microcirculation, normalization of colloid-osmotic pressure in microvessels, the development of hypocoagulation, a decrease in blood viscosity, a decrease in tissue edema, stimulation of regenerative processes, activation of fibrinolysis, local mechanisms of immunological defense, and increased sensitivity of microflora to antibiotics [48, 49]. Indications for magnetic laser therapy are all stages of the disease.
Low-frequency alternating magnetic field magnetic therapy (AMF) has become widespread in clinical practice. A study of the effect of low-inductance PeMF on the human body showed that it causes activation of compensatory homeostasis systems; the identified hypocoagulative effect has a beneficial effect on microcirculatory processes and regional blood circulation. PeMP has analgesic, anti-edematous and anti-inflammatory effects. Exposure to magnetic fields does not cause the formation of endogenous heat, an increase in temperature and skin irritation. This allows them to be used at any stage and form of the disease. The effect of PeMP is due to a change in membrane permeability, stimulating the formation of T- and B-lymphocytes with receptors for immunoglobulins of classes A and E. Thus, the activity of the cellular and humoral immunity is enhanced, which leads to hyposensitization and weakening of allergic reactions [50].
Of particular note is the positive influence of “running” magnetic fields, the spatial heterogeneity of which causes the formation of magnetic hydrodynamic forces in electrically conductive moving media (blood, lymph), which contribute to increasing the tone of venules, accelerating the diffusion of water dipoles, reducing edema, and stimulating lymphatic drainage. According to the literature, adding a low-frequency “traveling” magnetic field to standard drug treatment and elastic compression increases the effectiveness of therapy, influencing the main pathogenetic links of the disease (improving microcirculation processes, enhancing lymphatic drainage and, as a consequence, anti-edematous and anti-inflammatory effects) and can be used for all its stages [51].
Ultraviolet irradiation (UVR) has a beneficial effect in complicated forms of lymphedema. The indication for its use is erysipelas of the skin of the leg. UVR causes dilation of arterioles and capillaries, an increase in the phagocytic activity of leukocytes, and an increase in the body’s overall resistance to adverse factors due to increased adaptive capabilities. The use of ultraviolet irradiation of autologous blood in patients with lymphedema is pathogenetically justified, since this method promotes tissue oxygenation, improvement of the rheological properties of blood, activation of the immune system and nonspecific resistance of the body [52].
LPG technology (endermotherapy) has become widespread. This technique involves mechanical action on the tissue of two rotating rollers; vacuum aspiration is used to capture the skin fold. This method allows you to effectively combat the manifestations of fibrosis and is often used in complex treatment after a course of CDT and surgical treatment [53].
A relatively new technique is kinesio taping, which has become widespread due to its active use in professional sports. The method involves applying applications of elastic tapes on an adhesive base. Kinesio taping helps eliminate swelling and align fascial tissues [54, 55]. In addition, according to the literature, the addition of kinesiotaping to known lymphatic drainage physiotherapeutic techniques (alternating pneumatic compression and underwater shower massage) increases the therapeutic effectiveness due to the combined effect on the main links in the pathogenesis of lymphedema [56].
In the absence of contraindications from the cardiovascular system, balneotherapy and hydrotherapy are indicated, the effectiveness of which is due to the effect of hydrostatic water pressure, chemical and physical factors, alternating different temperatures on the lymphatic and blood vessels of the microvasculature [8].
In order to stimulate blood circulation, improve arterial blood flow, venous and lymphatic drainage, enhance metabolic processes, oxygen absorption by tissues, enzymatic activity, reduce perivascular edema, reduce platelet aggregation and blood viscosity, activate redox and immune processes, stimulate repair, increase bactericidal activity Hydrogen sulfide, radon and siliceous baths are used for skin treatment [50]. Underwater shower massage stimulates the process of lymphatic drainage, improves blood circulation, microcirculation, reduces hypoxia and improves tissue trophism.
In recent years, positive data have been obtained on the effective use of thalassotherapy in patients with lymphedema (therapy with sea water, therapeutic mud and algae). It has been established that the addition of thalassotherapy methods (cold algae wraps) to standard drug treatment and elastic compression increases the effectiveness of conservative treatment of patients with lymphedema due to the influence of biologically active components of brown seaweed, helping to improve microcirculation processes, lymphatic drainage function, peripheral hemodynamics, which leads to a decrease in hypoxia and improvement of tissue trophism [57, 58].
Positive results from the use of peloid therapy were noted. It has been established that adding silt sulfide peloids of indifferent temperature to standard drug treatment and elastic compression increases the effectiveness of complex conservative therapy for patients with lymphedema due to the influence of the biologically active components of therapeutic mud on improving microcirculation processes and enhancing lymphatic drainage function [59].