Medical information is reliable Checked by Eremin Alexey Valentinovich
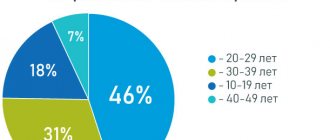
Treatment of anxiety personality disorder in Moscow, as in any large city, is relevant. This deviation is characterized by a person’s reluctance to communicate, a feeling of being an inferior person and high sensitivity to criticism directed at him. Social withdrawal in this case is caused by the fear of being ridiculed or humiliated. The disease takes various forms and manifests itself between the ages of 18 and 24 years. At the same time, concomitant disorders appear. Diagnosis is carried out using testing. Psychotherapy and medications are used to provide assistance.
Understanding Anxiety Disorders
At the beginning of the development of the disease, close people notice in a patient with an anxiety disorder his reluctance to communicate with peers and relatives. Then other manifestations of the disorder begin, which persist throughout the rest of life. The extent of its prevalence is difficult to assess, since patients rarely seek timely help. Treatment for anxiety personality disorder is usually carried out by psychiatrists, clinical psychologists and psychotherapists.
Almost always, with this disorder, other mental abnormalities are noted:
- panic disorder;
- agoraphobia;
- social phobia;
- obsessive-compulsive disorder.
Service price
- HOSPITAL Day hospital5 000
- Day hospital with intensive care8,000
- 24-hour hospital (all inclusive, cost per day) 12,000
- 24-hour hospital (all inclusive, cost per day). Single occupancy24,000
- 24-hour hospital (all inclusive, cost per day). Single occupancy in a superior room 36,000
- Primary family counseling for relatives of patients undergoing inpatient treatment free of charge
- Group psychotherapy for relatives of patients undergoing inpatient treatment free of charge
- Group psychotherapy for 24-hour and day hospital patients free of charge
- Individual post for a hospital patient (if indicated)6,000
Causes of development of anxiety personality disorder
Treatment of anxiety personality disorder is impossible without understanding the cause of the disease. Currently, modern science does not have enough information to clearly formulate the etiology. But it has already been noted that several factors are involved in the emergence of the problem, including genetic predisposition, character traits, temperament, surrounding society and upbringing.
Even in childhood, a tendency to anxiety disorder manifests itself as a child’s poor adaptation to a complex and rapidly changing situation, fearfulness and isolation. But you need to understand that some shyness and timidity when contacting others can act as a normal part of the process of mental development, and has nothing to do with the disease. Normally, this phenomenon goes away over time, but with anxiety disorder, problems with communication and avoidance of contacts persist.
Experts point to the fact that most patients grew up and developed in a family where they were constantly criticized, rejected and not taken seriously. For a child, his parents are always significant people, and therefore the psychotrauma associated with improper upbringing has a strong impact on a person’s future life. A long stay in the absence of emotional intimacy leads to the desire to move away from loved ones.
Cure prognosis
TDR of physiological etiology is easily eliminated during the treatment of the underlying disease, with the exception of irreversible forms of brain damage. The difficulty is in the treatment of anxious depression caused by personal and psychological factors. In this case, early intervention and the assistance of the patient’s immediate environment play a decisive role.
Carrying out a full course of complex therapy helps to remove anxiety and normalize the general emotional mood, but to ensure the absence of relapses, patients are recommended to work on developing stress resistance so that an unexpected “blow of fate” does not provoke a new attack of anxiety and depression.
Share this article
Symptoms of Anxious Personality Disorder
Before you begin treatment for an anxious personality disorder, you should accurately identify all the symptoms of this pathology. You can already notice some deviations from the norm in a small child. This usually manifests itself this way:
- timidity;
- shyness;
- fear of new acquaintances;
- difficulty answering at the board;
- reluctance to be the center of attention;
- severe discomfort in an unusual situation.
The patient prefers to spend time alone, watch movies, read books and fantasize. His social circle is small and consists mainly of relatives. Constantly keeping strangers at a distance is not due to a lack of need for social contacts, but to the fear of making oneself a laughing stock, of being humiliated and rejected. For such a person, even completely neutral statements from people can cause a strong negative reaction and be perceived as a personal insult.
At the same time, the patient experiences a strong need for emotional intimacy, but he can accept it only under the condition of complete acceptance and goodwill. Even the most insignificant deviation from a gentle atmosphere turns into a tragedy for the patient, evidence of humiliating rejection. For this reason, they often remain lonely. Treatment for anxiety personality disorder should begin as early as possible, since the lack of help will greatly reduce the quality of life of such a person.
When trying to establish contact, a patient with such a disorder experiences great awkwardness and tension. He is not characterized by spontaneity; from the outside he looks shy, clumsy and incomprehensible. Some patients with this disorder, in an attempt to establish communication, may ingratiate themselves with others, and some of them may simply avoid any new acquaintances. They expect constant humiliation, and with their behavior they provoke society into displaying negativity. And this leads to even greater isolation.
Avoidant behavior not only leads to problems in your personal life. It is impossible to build a career under such conditions. A person with an anxiety disorder cannot make professional connections, speak in front of large numbers of people, lead others, or take full responsibility for their decisions. They usually remain in the role of a quiet and inconspicuous subordinate, have difficulty changing their place of residence and work, and rarely make friends among colleagues.
If a patient ends up in a team where he is treated negatively, then this situation leads to rapid decompensation of his condition. Attempts to relieve tension with the help of alcohol or psychoactive substances in such individuals end in addiction to alcohol and drugs.
Prevention
The best “soil” for neuroses and depression is a poor psychological climate in the family, at work, and the lack of a healthy balance of neuropsychic and physical stress.
There are no specific preventive measures for neurosis. If you take care of your mental health and adhere to a healthy lifestyle, even if you have a genetic predisposition, a mental disorder will not become active. General recommendations:
- engage in education on the topic of mental health, neuroses and depression - this is important for developing the ability to identify mental pathology in a timely manner;
- have a hobby that helps you take your mind off stress for a while;
- adhere to a normal work-rest, sleep-wake schedule;
- if there are family conflicts, contact a psychologist for their timely resolution;
- It is not recommended to close yourself off from people too much - you should at least sometimes spend time with friends, visit clubs of similar interests;
- prevent traumatic influences at work and in the family.
Diagnosis of Anxious Personality Disorder
Treatment of anxiety personality disorder in Moscow at Dr. Isaev’s clinic is carried out only after an accurate diagnosis has been established. To do this, the doctor conducts a conversation with the patient and then evaluates the results of psychological testing. The following identified signs are considered diagnostic criteria in this case:
- constant pressure;
- confidence in one's low value to society;
- constant worry about the opinions of others;
- rejection of criticism;
- reluctance to enter into a relationship when there is no confidence in the person’s sympathy;
- the presence of restrictions in professional and social work.
Identification of an anxiety disorder is carried out after receiving all the examination data and making a differential diagnosis with other mental disorders. Similar symptoms are observed in the following diseases:
- social phobia;
- dependent disorder;
- psychopathy of schizoid type;
- histrionic or borderline personality disorder.
Treatment of social phobia is carried out when a person is not afraid of communicating with another person, but simply cannot tolerate certain social situations. Treatment of psychopathy is carried out under the condition of fear of approaching strangers due to fear of loss of identity. Dependent disorder is characterized by the presence of a phobia of separation, rather than the contact and criticism itself. If a person's behavior is marked by attempts at manipulation and a violent reaction to a negative attitude, then this phenomenon is not considered anxiety, and treatment for hysteria or borderline disorder is carried out.
Literature
- Karavaeva T.A. Principles and algorithms of psychotherapy for anxiety disorders of a neurotic level // St. Petersburg Research Psychoneurological Institute named after. V.M. Bekhterev", 2021.
- Generalized anxiety disorder: clinical recommendations // Developer of clinical recommendations: Russian Society of Psychiatrists, 2015.
- Zabylina N. A. Issues in the diagnosis of mixed anxiety and depressive disorder // Journal of Siberian Medical Sciences, 2008.
- Shitov E. A. Neurotic and somatoform disorders: guidelines for students in the discipline “Psychiatry” // State Budgetary Educational Institution of Higher Professional Education Ryaz State Medical University of the Ministry of Health of Russia. – Ryazan: RIO Ryaz State Medical University, 2013.
Treatment of anxiety personality disorder in Moscow
Dr. Isaev’s clinic treats anxiety personality disorder using an individual approach to each person. The patient receives therapy on an outpatient basis. Usually it is successful, this is due to the selection of the most effective methods. The most common methods of psychotherapy in this case are:
- cognitive-behavioural;
- psychoanalytic;
- social skills training;
- individual and group therapy.
The techniques that underlie cognitive behavioral therapy help to detect the presence of distortions of expectations, create a change in thinking and interpretation of events, and teach easy and free communication. Psychoanalysis allows the patient to become aware of his internal conflicts and the reasons for their occurrence, and to reconsider his life in a new light. The main task of a specialist is to help a person overcome his greatly exaggerated fears about his own inadequacy.
The difficulty of working with a patient lies in his tension and constant expectation of rejection. It can be difficult to build a trusting relationship with such a person. When a person begins to talk about his problems, he unconsciously tries to please his psychologist or psychotherapist and find approval for his actions and thoughts. If the patient suddenly decides that he is not understood or is being judged, he stops being frank and immediately closes down. In this case, therapy can be interrupted at the client’s request.
A distinctive feature of a person with an anxiety disorder is his stories about the fear of gossip about him, while he does not express a desire to learn to accept reality. Often the patient has several disorders at once; along with anxiety, he suffers from social and other types of phobia. And all this should be taken into account when prescribing the type of therapy.
The greatest benefit for anxiety disorders comes not so much from individual sessions as from group sessions. There, a person feels in his own environment and can quickly develop communication skills, since the specialist always maintains a warm and friendly atmosphere within the group. It is she who helps relieve stress from the patient.
Treatment of an anxious personality disorder is considered complete at the moment when a person’s new behavior is firmly established. With the right approach, the prognosis for this disease is usually favorable. The forecast for recovery is less optimistic if the disease is complicated by other severe mental disorders.
Pharmacotherapy for anxiety disorder in its pure form is rarely used. It is used as an adjunct, if necessary, for the treatment of depression or other disorders that interfere with acquiring socialization skills and changing behavior.
Over the past decade, there has been a significant increase in interest in psychopathological conditions, the clinical picture of which is determined by anxiety. In our country, these conditions have traditionally been considered within the framework of affective disorders, neuroses and psychogenic reactions. However, scientific data accumulated during the 70-80s indicate the need to revise traditional nosological views and allocate anxiety disorders into a separate diagnostic category [1,2]. It usually includes panic disorder, various types of phobias, generalized anxiety disorder, obsessive-compulsive disorder, and disorders associated with mental stress. Adjacent to this category is a large group of shallow mental disorders characterized by so-called subsyndromal anxiety.
Epidemiological studies show that anxiety disorders are the second most common group of mental disorders after mood disorders. Their prevalence in the population ranges from 6% to 13.6%. [3]. At the same time, they have a huge impact on disability and quality of life [4].
Since anxiety is a universal psychophysiological phenomenon associated with adaptation to stress, it is important to distinguish between normal (adaptive) and pathological anxiety [5, 6].
Normal anxiety can be defined as a feeling of emotional discomfort caused by uncertain prospects. It is associated with a threatening situation, intensifies with an increase in its subjective significance, and increases under conditions of a lack of time and information. Adaptation anxiety, as a rule, is short-lived and does not reach excessive strength that interferes with activity (Table 1).
Anxiety is a universal psychophysiological phenomenon associated with adaptation to stress
Pathological anxiety can also be provoked by external circumstances, but its occurrence is largely determined by internal reasons. Pathological anxiety is not associated with a real threat and is inadequate to the significance of the situation.
An important difference between pathological anxiety is its strong severity. Therefore, painful anxiety causes severe subjective experiences, leads to a decrease in productive activity and often takes over consciousness. In addition, pathological anxiety usually manifests itself in the form of specific psychopathological syndromes.
Table 1. Differences between adaptive and pathological anxiety
| Normal (adaptive) anxiety | Pathological anxiety |
| Due to a real external threat | Caused by internal reasons, but can be provoked by external circumstances |
| Increases in conditions of significance of choice | Not adequate to the real significance of the situation |
| Increased by lack of information | Does not depend on objective information |
| Strengthens when there is a lack of time, helps speed up decision making | Blocks constructive decision making |
| Can be controlled and suppressed by the subject himself | Is not amenable to subjective control, takes over consciousness |
| Subjectively experienced as a natural reaction to a situation | Subjectively experienced as excessive and inadequate, has specific clinical manifestations |
Detailed psychopathological qualification of these syndromes is often difficult and requires the involvement of psychiatrists. However, in most cases, to determine medical tactics, it is enough to establish only the type of pathological anxiety. There are two such types: paroxysmal and constant [1]. Each of these types can be divided into several subtypes that correspond to the main nosographic groups of anxiety disorders.
The main distinguishing features of paroxysmal anxiety are the episodic occurrence and intensity. A typical attack is characterized by rapidly growing anxiety, which turns into fear, accompanied by a large number of autonomic disorders and unpleasant bodily sensations. [6,7]. Panic anxiety is usually experienced as a feeling of immediate threat to the individual’s existence or the integrity of his “I”. Patients experiencing such anxiety complain of inexplicable fear, a feeling of approaching death, or a feeling of loss of sanity. Their behavior at the time of the attack is characterized by inhibition or uncoordinated and limited arousal - panic.
The physiological mechanisms of paroxysmal anxiety are associated with pathological activation of the hypothalamus and vegetative centers of the brain stem, which determines polymorphic vegetative symptoms, as well as unpleasant bodily sensations, which the doctor pays attention to first when contacting such a patient. However, it should be borne in mind that in the genesis of paroxysmal anxiety, the overlying structures of the brain also play an important role - the limbic system, hypothalamus, amygdala, septum, hippocampus, prefrontal cortex, etc. [8].
In social phobia, fear is associated with situations of interpersonal contact. The main experience is the fear of being in a humiliating or awkward position.
Disorders that cause anxiety attacks include panic disorder, agoraphobia, social phobia, and specific phobia. All of these disorders are characterized by anxiety attacks, which can occur spontaneously (as in panic disorder) or in response to some stimulus. Depending on the stimulus that provokes an anxiety attack, various types of phobias are distinguished. With agoraphobia, anxiety is provoked by situations in which the patient feels alone and cannot get the necessary help in case of illness. Usually this feeling occurs in confined spaces, when moving away from home, in a crowd, or when it is necessary to be alone. Agoraphobia typically develops in people who already have panic disorder or have had isolated panic attacks in the past.
In social phobia, anxiety attacks are associated with situations of interpersonal contact, or the need to act in the presence of other people (so-called performance phobias). The main experience that occurs in such patients is the fear of being in a humiliating or awkward position.
With a specific phobia, anxiety attacks occur upon contact with certain objects or situations specific to each patient. Most often, such irritants are animals or insects (dogs, spiders, etc.), natural phenomena (thunderstorm, hurricane, etc.), the sight of blood, injections, as well as certain circumstances (flying on an airplane, riding in an elevator, etc.). ).
The most important signs of phobias, in addition to the connection of paroxysmal anxiety with a specific stimulus, also include the patient’s avoidance of this stimulus. This phenomenon is usually referred to as avoidant or restrictive behavior.
Disorders accompanied by paroxysmal anxiety are very common. Table 2 shows their lifetime prevalence rates [1]. The medical significance of these disorders is due, first of all, to the difficulties of differential diagnosis. Compliance issues are also of great importance, especially in cases where patients, due to anxiety, avoid visiting the doctor, do not comply with the regimen, or do not take medications.
Table 2. Lifetime prevalence in the population of disorders accompanied by paroxysmal anxiety
| Disorders | Lifetime frequency (%) |
| Panic disorder | 1,7 – 2,9 |
| Agoraphobia | 0,7 – 1,1 |
| Social phobia | 3,5 – 6,7 |
| Specific phobia | 7,2 – 11,3 |
Constant anxiety
A distinctive feature of this type of anxiety is its constant presence over a long period of time. [9, 10, 11]. Constant anxiety, like paroxysmal anxiety, is closely related to autonomic arousal, but this relationship is not expressed to the same extent. Therefore, autonomic symptoms do not necessarily occupy a large place in the clinical picture. Persistent anxiety is usually experienced as worry or worry about upcoming events or their consequences. This type of anxiety in different disorders has its own clinical characteristics, which are discussed below.
The mechanisms of constant anxiety, as well as paroxysmal anxiety, are associated with the limbic system, amygdala, septum and hippocampus. However, in its genesis, the prefrontal cortex and brain systems responsible for the perception of exteroceptive stimuli (thalamus, somatosensory, auditory and visual cortex) seem to play a larger role [12, 13]. There is evidence of a close connection between persistent anxiety and cognitive impairment, which is especially noticeable in the initial subclinical stages of dementia.
Persistent anxiety occurs in generalized anxiety disorder, adjustment disorders, stress disorders, as well as in a number of other conditions encountered in medical practice.
Patients with generalized anxiety often show signs of increased autonomic arousal, which is expressed in tachycardia, sweating, dry mucous membranes, difficulty breathing, nausea, chills, gastrointestinal and other somatic symptoms
The main symptom of generalized anxiety disorder is excessive chronic anxiety, which is supported by constantly arising anxious expectations and worries. This concern arises for various unrelated reasons (for example, due to family, economic situation, work, health, etc.). These reasons are of an everyday nature, often replacing each other or coexisting. At the same time, the readiness for anxiety remains even when the events that bothered the patient are safely resolved. Patients with generalized anxiety disorder usually recognize the excessiveness of their anxiety, as well as their inability to cope with it on their own. At the same time, they believe that these unrest have real grounds.
In addition to anxious expectations, with generalized anxiety there are disturbances in the sleep-wake cycle, as well as an increase in general excitability. Patients with generalized anxiety disorder report a feeling of internal tension, combined with increased fatigue, irritability, impaired concentration and sleep disorders. Generalized anxiety disorder is also accompanied by psychomotor symptoms. Patients experience fussiness and restlessness, an inability to physically relax, as well as increased muscle tone. Against this background, tension headaches, back pain, the symptom of “restless” legs, tremors and other similar manifestations may be observed.
Patients with generalized anxiety often show signs of increased autonomic arousal, which is expressed in tachycardia, sweating, dry mucous membranes, difficulty breathing, nausea, chills, gastrointestinal and other somatic symptoms. However, these signs are currently not considered by most specialists as necessary for making a diagnosis of generalized anxiety disorder.
Persistent anxiety is often noted in disorders caused by mental stress. The most common type of such conditions are adaptation disorders. Disorders of mental activity in these cases develop after significant or subjectively significant changes in a person’s life (moving, changing marital status, industrial or academic failures, the onset of a disease, etc.). These disorders are usually short-lived, but sometimes they can last for several months or even years. For many patients, constant anxiety comes to the fore. It manifests itself in doubts, hesitations, fears about the future, as well as prolonged psychophysical stress. Disorders of appetite and increased fatigue are typical, and sometimes explosiveness, moodiness, suspiciousness or wariness are noted. These conditions are often accompanied by autonomic disorders in the form of arterial hypertension or digestive disorders. Headaches and other somatic symptoms may occur.
A special subgroup of conditions accompanied by constant anxiety are stress disorders. These disorders occur when exposed to extreme mental trauma, i.e. in situations involving the threat of death or serious physical harm to the subject himself or to other people. Currently, it is common to distinguish between acute stress disorder and post-traumatic stress disorder. Typically, acute stress disorder refers to psychopathological conditions that developed during or immediately after exposure to mental trauma and lasted from 2 days to 4 weeks[2]. If the stress disorder continues for more than 1 month, then we should talk about the formation of post-traumatic stress disorder (PTSD). And if it continues for more than 3 months, then this disorder enters the chronic phase. It is important to note that PTSD can occur long after the stress has occurred.
Although constant anxiety underlies stress disorders, it does not always come to the fore in the clinical picture. The clinical picture of these disorders is determined by a wide range of states of altered consciousness and self-awareness (mental numbness or emotional anesthesia, a feeling of detachment, depersonalization-derealization phenomena, amnesia). These phenomena are usually combined with intrusive (i.e., invading consciousness) symptoms in the form of recurring thoughts, images, dreams, illusions, experiences and overwhelming ideas. This also includes signs of increased mental sensitivity and avoidance of stimuli reminiscent of the stress experienced. Another sign of a stress disorder is a persistent increase in excitability. This is expressed in difficulties falling asleep and intermittent sleep, fearfulness, irritability, outbursts of anger, difficulty concentrating, and mood swings. Post-traumatic stress disorder is characterized by the appearance of persistent vegetative shifts and general changes in the body's reactivity.
Constant anxiety is often observed in other mental disorders, a description of the clinical features of which is impossible in this work due to the limited scope. However, it should be noted that this type of anxiety, as a rule, accompanies persistent vegetative changes, which are presented to general practitioners in the form of functional somatic disorders (for example, thermoneurosis, psychogenic shortness of breath, “stress” gastritis, irritable bowel syndrome, idiopathic urticaria, etc.) , as well as eating disorders, sexual disorders and insomnia of a non-organic nature. In many such cases, we are talking about subsyndromal anxiety, manifested by chronic tension, inability to relax, apprehension, increased excitability, irritability and fatigue. And, although an unambiguous nosographic classification of these conditions can be very difficult, therapeutic approaches are in many ways similar to those used for other forms of persistent anxiety.
Persistent anxiety is quite common [1] (Table 3). It is especially often detected in patients with somatic diseases. Thus, the frequency of generalized anxiety disorder in coronary heart disease reaches 24% [14], and in diabetes mellitus it ranges from 14% to 40% [15, 16]. 18–40% of trauma patients develop clinically defined PTSD [17, 18], as do a large number of people who have undergone cardiac surgery [19]. At the same time, symptoms of anxiety may resemble signs of corresponding diseases and affect the patient’s general well-being and quality of life.
Table 3. Lifetime prevalence in the population of disorders accompanied by persistent anxiety
| Disorders | Lifetime frequency (%) |
| Generalized anxiety disorder | 4,2 – 6,6 |
| Post-traumatic stress disorder | 7,8 – 9,2 |
Psychopharmacotherapy of pathological anxiety
Pharmacological therapy for anxiety disorders is currently based on the use of two classes of drugs: antianxiety drugs and antidepressants. In turn, among anti-anxiety drugs, benzodiazepine tranquilizers (BZD) and hydroxyzine (Atarax) should be mentioned, and among antidepressants, selective serotonin reuptake inhibitors (SSRIs).
Benzodiazepines
The advantages of BZDs are their high anti-anxiety activity, good tolerability, and the rapid onset of a therapeutic effect. The negative aspects of the action of BZD are associated with the risk of dependence, sedation, impairment of cognitive processes and an increase in tolerance. With abrupt withdrawal of drugs from this group, a rebound syndrome usually occurs, which is expressed in increased mental manifestations of anxiety and its vegetative accompaniment. In the presence of physical dependence, a withdrawal syndrome appears, which is characterized by severe anxiety, sleep disturbances, nausea, headaches, dizziness, increased sensitivity to light and noise, tremors, increased body temperature, fluctuations in blood pressure, convulsions and changes in consciousness up to delirium.
Constant anxiety is very common and is especially often detected in patients with somatic diseases
The use of BZDs for anxiety disorders should be very limited and, if possible, limited to only occasional use for paroxysmal anxiety, in particular, for the relief of anxiety attacks. Their short-term use for acute stress anxiety is reasonable (but not uncontroversial).
BZD should not be prescribed to patients with a history of substance abuse or personality disorders. The use of BZD should be avoided in cases of persistent anxiety, especially in generalized anxiety disorder, adjustment disorders, PTSD and subsyndromal anxiety. The use of these drugs in these cases leads to unreasonable escalation of doses, impairment of cognitive functions, addiction, and motor impairment [20].
Hydroxyzine (Atarax)
Hydroxyzine began to be actively used for the treatment of anxiety relatively recently. According to its neurochemical properties, it is an antagonist of H1-histamine receptors. This drug also has low anticholinergic activity. The mechanisms of its action remain unexplored. However, the therapeutic effects of hydroxyzine are not limited to the effect on the histamine system, since under experimental conditions this drug exhibits an anti-anxiety effect similar to the action of fluoxetine, imipramine and chlordiazepoxide and does not coincide with the effect of another typical H1-histamine receptor antagonist, chlorpheniramine [21].
Hydroxyzine has proven to be a very effective treatment for chronic anxiety and, primarily, in the treatment of generalized anxiety disorder. It also has high activity against prolonged adjustment disorders and persistent subsyndromal anxiety. There is evidence that hydroxyzine reduces the number of panic attacks in panic disorder and may also help normalize sleep. It can be successfully used for various conditions characterized by prolonged psycho-vegetative stress. The beneficial properties of hydraxizine in the treatment of somatic manifestations of anxiety are its antiemetic effect and antipruritic effect.
The psychopharmacological action of hydroxyzine consists of two phases. In the first phase (within 5-8 days), a general sedative effect, characteristic of many antihistamines, predominates. This period may be accompanied by a number of side effects (drowsiness, lethargy, weakness), apparently due to the direct antihistamine effect. The second phase, usually starting from 6 to 9 days of therapy, is characterized by the gradual disappearance of the phenomenon of sedation and an increase in anti-anxiety and vegetative-stabilizing effects. An important feature of the action of hydroxyzine, which distinguishes it from benzodiazepines, is its positive effect on memory and attention [22, 23].
The advantage of hydroxyzine compared to benzodiazepines is the lack of development of tolerance to its anxiolytic effect, even with long-term use. When you stop taking this drug, there is no withdrawal syndrome or rebound symptoms. Unlike benzodiazepines, its use does not develop dependence. Hydroxyzine does not have euphoric properties. And after abruptly stopping taking this drug, a gradual increase in anxiety is observed only after 3-5 days.
Antidepressants
There are several groups of antidepressants, many of which are successfully used in the treatment of anxiety disorders. However, until recently, antidepressants—selective serotonin reuptake inhibitors (SSRIs)—remain the first choice drugs. Drugs in this group are indicated primarily for paroxysmal anxiety (panic disorder, agoraphobia, social phobia, some cases of specific phobia). In addition, they have proven effective in cases of severe persistent anxiety (post-traumatic stress disorder and generalized anxiety).
When prescribing SSRIs, it is necessary to keep in mind the transient increase in anxiety that is often noted during their prescription (the so-called initial anxiety), the appearance of gastrointestinal discomfort, sleep disturbances, as well as the suppressive effect of these drugs on sexual function and appetite. There is information about an increase in body weight under their influence, as well as cases of withdrawal syndrome. In addition, possible drug interactions due to the inhibitory effect of SSRIs on the liver enzyme system—cytochrome P450—should be taken into account [24].
For anxiety disorders, other drugs (sedatives, antipsychotics, anticonvulsants) are sometimes successfully used.
A clinically significant problem is the choice between different drugs in this category. Since various SSRIs are approximately the same in their pharmacological activity, their selection in the treatment of pathological anxiety should be based on the spectrum of side effects, as well as the relationship between stimulant and sedative properties. There is still little reliable information on this matter. However, given the literature and clinical experience, some preliminary guidelines can be used.
Thus, according to the severity of the sedative effect, SSRIs can be distributed as follows: Fluvoxamine => Paroxetine => Sertraline => Citalopram => Fluoxetine.
According to the ability to provoke initial anxiety: Fluoxetine => Sertraline => Paroxetine => Citalopram => Fluvoxamine.
According to the ability to cause withdrawal symptoms: Paroxetine => Sertraline => Citalopram => Fluvoxamine => Fluoxetine
By overall incidence of side effects: Fluvoxamine => Fluoxetine => Paroxetine => Sertraline => Citalopram
As for side effects, the most common for citalopram are headache, dry mouth, tremor, dizziness and sweating. Sometimes there is increased drowsiness; in case of overdose, a pronounced cardiotoxic effect is possible.
Side effects of fluoxetine include headache, rash, psychomotor agitation, akathisia, sleep disturbances and appetite suppression. In addition, this drug has the longest half-life, which on the one hand reduces the possibility of withdrawal syndrome and allows its use in patients with low compliance. On the other hand, fluoxetine therapy requires a longer period to establish equilibrium concentrations and produce a therapeutic effect.
When prescribing fluvoxamine, nausea, diarrhea, dizziness and tremor are most often observed. The named drug has a pronounced sedative effect, but it has almost no effect on sexual functions and does not lead to an increase in body weight.
Paroxetine is more likely to cause sexual dysfunction, sweating and weight gain. It has a fairly pronounced sedative effect. It can also cause constipation. And when stopping treatment with paroxetine, withdrawal syndrome occurs more often than with other SSRIs.
Sertraline has the ability to cause diarrhea, headache, dizziness and tremors, disrupt sleep and cause sexual dysfunction. This drug is the only one in this group that does not cause an increase in prolactin.
Along with these groups of drugs, other drugs (sedatives, antipsychotics, anticonvulsants) are sometimes successfully used for anxiety disorders. However, the positive effect obtained with their help in one patient cannot always be reproduced in another. In some cases, these drugs have low pharmacological activity or have serious side effects. Therefore, their use is not considered in this work.
[1] Other types of anxiety (for example, obsessive and psychotic) are much less common in general practice.
[2] This work uses the criteria for stress disorders of the American Classification of Mental Disorders - DSM-IV-TR. ICD-10 uses slightly different time criteria, however, the principle of taxonomy of stress disorders is the same.
Questions and answers
Which doctor should you see for an anxiety disorder?
This disease is a variant of the manifestation of neurosis. That's why a psychotherapist deals with it. It can be successfully treated using different methods, but to choose the most effective therapy you need to visit a specialist.
Is it possible to cope with anxiety forever?
An anxiety disorder that is not complicated by comorbid conditions can usually be treated successfully. It is important that a person makes an effort and has the motivation to get rid of the problem.
Treatment options
Comprehensive treatment of anxiety and depressive disorders, including psychotherapy, physiotherapy and medication, has proven to be the most effective.
Psychotherapy
The best results in the treatment of anxious depression are demonstrated by cognitive behavioral psychotherapy, during which the doctor teaches patients the skills of in-depth analysis of their views, which allows patients to independently identify erroneous illogical reasoning, and also helps to form correct behavioral stereotypes.
Other types of psychotherapy used to treat SDD include:
- Gestalt therapy . The patient is taught the ability to lead a fully conscious life, due to which most unconscious destructive experiences are deprived of the chance to develop.
- Family psychotherapy . Correction of the mental state is achieved by improving the family atmosphere. Most applicable for the treatment of anxious depression in children and adolescents.
- Hypnotic suggestion . The doctor gives the patient the necessary settings for subsequent correction of erroneous forms of behavior.
Drug treatment
Depending on the form of TDR, the patient may be prescribed the following groups of drugs:
- Antidepressants . Effective in treating apathy and feelings of hopelessness, improve overall emotional mood, normalize sleep and appetite.
- Beta blockers . Indicated for severe forms of somatic disorders.
- Tranquilizers . They help reduce the intensity of feelings of fear and anxiety, reduce the frequency of panic attacks, and eliminate most somatic disorders.
Physiotherapy
To improve brain activity and general well-being, patients are prescribed massage, as well as certain physical procedures:
- Electrosleep . Removing foci of increased excitation in the cerebral cortex by using low-frequency electric current.
- Electroconvulsive therapy . Simulation of brain activity by electric current discharges of a given intensity.
- Darsonval . Treatment of the scalp with a weak high-frequency current to improve blood circulation.
- Oxygen therapy . Inhalation of pure oxygen (O₂) to quickly stimulate blood circulation in the brain and improve the general condition of the patient.
- Acupuncture . Stimulation of certain reflexogenic zones to improve the functioning of specific internal organs and systems or the general health of the entire body.
Why does the disorder occur?
Doctors cannot give an exact answer to the question posed - they do not know the reliable mechanisms of occurrence of the described pathological process. But, some scientists argue that it has a cognitive origin, that is, obsessive experiences appear due to a distortion of a person’s stereotypical thinking.
According to A. Beck, an American psychotherapist, professor at the University of Pennsylvania and creator of cognitive psychotherapy, anxiety is a normal reaction to upcoming changes and danger, but there are individuals whose assessment of the development of the situation is distorted due to low self-esteem. It is because of self-doubt that they subconsciously believe that they will not be able to cope with a dangerous situation, as a result of which this pathology develops.
Causes
Today there is no clear opinion about the causes of this disorder. It is believed that the formation of anxious (avoidant) personality disorder is influenced by genetic, psychological and social factors. Features of temperament that have a hereditary basis, as well as accentuation of character, are undoubtedly a predisposing factor.
A situation of chronic stress in childhood in the form of constant criticism and rejection from parents with age can develop into this personality disorder as a way of psychological protection from emotionally painful situations of rejection.
First symptoms and signs
An uncontrollable feeling of anxiety that lasts for at least six months without objective reasons is the main symptom of an anxiety disorder. Anxiety can be so strong that the patient’s life changes dramatically. A person will not be able to leave the house, work, or communicate with loved ones. Anxiety may subside for a few hours, days or weeks, but any minor reason will cause it to return again.
Physiologically, the following symptoms may appear:
- constant feeling of fatigue;
- disturbed sleep;
- persistent fear;
- inability to concentrate on any task or relax;
- trembling in hands;
- nervousness;
- rapid heartbeat in the absence of heart problems;
- dizziness;
- excessive sweating;
- headache and muscle pain.