Today, in the era of high development of information technology and, thereby, active popularization of knowledge about various diseases of the population, incl. During pregnancy, improving family planning methods, it is relevant to increase the knowledge of women planning pregnancy about the risk of developing gestational diabetes mellitus in order to timely seek medical help in highly qualified medical institutions, where this problem is dealt with by doctors with extensive clinical experience in managing such patients.
basic information
Gestational diabetes mellitus, which develops during pregnancy, is characterized by hyperglycemia (increased blood glucose levels). In some cases, this disorder of carbohydrate metabolism may precede pregnancy and be first identified (diagnosed) only during the development of this pregnancy.
During pregnancy, physiological (natural) metabolic changes occur in the mother's body, aimed at the normal development of the fetus - in particular, the constant supply of nutrients through the placenta.
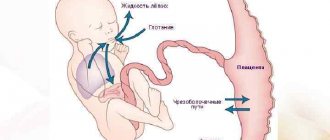
The main source of energy for the development of the fetus and the functioning of the cells of its body is glucose, which freely (through facilitated diffusion) penetrates the placenta; the fetus cannot synthesize it on its own. The role of the conductor of glucose into the cell is played by the hormone “insulin”, which is produced in the β-cells of the pancreas. Insulin also promotes the “storage” of glucose in the fetal liver.
Amino acids - the main building material for protein synthesis in the fetus, necessary for cell growth and division - are supplied in an energy-dependent way, i.e. through active transfer across the placenta.
In the mother’s body, to maintain energy balance, a protective mechanism is formed (“rapid starvation phenomenon”), which implies an immediate restructuring of metabolism - preferential breakdown (lipolysis) of adipose tissue, instead of the breakdown of carbohydrates with the slightest restriction in the supply of glucose to the fetus - ketone bodies (products) increase in the blood fat metabolism are toxic to the fetus), which also easily penetrate the placenta.
From the first days of physiological pregnancy, all women experience a decrease in fasting blood glucose levels due to accelerated excretion in the urine, decreased glucose synthesis in the liver, and glucose consumption by the fetoplacental complex.
Normally, during pregnancy, fasting blood glucose does not exceed 3.3-5.1 mmol/l. The blood glucose level 1 hour after eating in pregnant women is higher than in non-pregnant women, but does not exceed 6.6 mmol/l, which is associated with a decrease in motor activity of the gastrointestinal tract and an increase in the absorption time of carbohydrates supplied with food.
In general, in healthy pregnant women, fluctuations in blood glucose occur within very narrow limits: on an empty stomach on average 4.1 ± 0.6 mmol/l, after meals - 6.1 ± 0.7 mmol/l.
In the second half of pregnancy (starting from the 16-20th week), the fetal need for nutrients remains highly relevant against the backdrop of even faster growth rates. The placenta plays a leading role in changes in a woman’s metabolism during this period of pregnancy. As the placenta matures, active synthesis of hormones of the fetoplacental complex occurs, which maintain pregnancy (primarily placental lactogen, progesterone).
As the duration of pregnancy increases, for its normal development in the mother's body, the production of hormones such as estrogens, progesterone, prolactin, cortisol increases - they reduce the sensitivity of cells to insulin. All these factors, against the background of decreased physical activity of the pregnant woman, weight gain, decreased thermogenesis, decreased insulin excretion by the kidneys, lead to the development of physiological insulin resistance (poor tissue sensitivity to its own (endogenous) insulin) - a biological adaptive mechanism for creating energy reserves in the form of adipose tissue in in the mother's body in order to provide nutrition to the fetus in case of starvation.
In a healthy woman, a compensatory increase in insulin secretion by the pancreas occurs approximately three times (the mass of beta cells increases by 10-15%) to overcome such physiological insulin resistance and maintain blood glucose levels normal for pregnancy. Thus, there will be an increased level of insulin in the blood of any pregnant woman, which is the absolute norm during pregnancy!
However, if the pregnant woman has a hereditary predisposition to diabetes mellitus, obesity (BMI more than 30 kg/m2), etc. The existing secretion of insulin does not allow overcoming the physiological insulin resistance that develops in the second half of pregnancy - glucose cannot penetrate the cells, which leads to an increase in blood sugar and the development of gestational diabetes mellitus. Through the bloodstream, glucose is immediately and unhinderedly transferred through the placenta to the fetus, facilitating its production of its own insulin. Fetal insulin, having a “growth-like” effect, leads to stimulation of the growth of its internal organs against the background of a slowdown in their functional development, and the entire flow of glucose coming from the mother to the fetus through its insulin is deposited in the subcutaneous depot in the form of fat.
As a result, chronic hyperglycemia of the mother harms the development of the fetus and leads to the formation of so-called diabetic fetopathy - fetal diseases that occur from the 12th week of intrauterine life until the onset of labor: high fetal weight; violation of body proportions - large belly, wide shoulder girdle and small limbs; advance of intrauterine development - with ultrasound, an increase in the main dimensions of the fetus in comparison with gestational age; swelling of the tissues and subcutaneous fat of the fetus; chronic fetal hypoxia (impaired blood flow in the placenta as a result of prolonged uncompensated hyperglycemia in a pregnant woman); delayed formation of lung tissue; trauma during childbirth.
Child health problems with gestational diabetes mellitus
Thus, at the birth of children with fetopathy, there is a violation of their adaptation to extrauterine life, which is manifested by the immaturity of the newborn even with a full-term pregnancy and its large size: macrosomia (child weight more than 4000 g), respiratory disorders up to asphyxia (suffocation), organomegaly (enlarged spleen, liver, heart, pancreas), heart pathology (primary damage to the heart muscle), obesity, jaundice, disorders in the blood coagulation system, the content of erythrocytes (red blood cells) in the blood increases, as well as metabolic disorders (low values of glucose, calcium , potassium, magnesium blood).
Children born to mothers with uncompensated gestational diabetes mellitus are more likely to experience neurological diseases (cerebral palsy, epilepsy); during puberty and thereafter, the risk of developing obesity, metabolic disorders (in particular, carbohydrate metabolism), and cardiovascular diseases is increased.
On the part of a pregnant woman with gestational diabetes mellitus, polyhydramnios, early toxicosis, urinary tract infections, and late toxicosis are more common (a pathological condition that is manifested by the appearance of edema, high blood pressure and proteinuria (protein in the urine), develops in the second and third trimester up to preeclampsia - cerebrovascular accident, which can lead to cerebral edema, increased intracranial pressure, functional disorders of the nervous system), premature birth, spontaneous abortion, delivery by cesarean section, labor anomalies, and trauma during childbirth are more common.
Disorders of carbohydrate metabolism can develop in any pregnant woman, taking into account the hormonal and metabolic changes that consistently occur at different stages of pregnancy. But the highest risk of developing gestational diabetes is in women who are overweight/obese and over 25 years of age; presence of diabetes in close relatives; with disorders of carbohydrate metabolism identified before the current pregnancy (impaired glucose tolerance, impaired fasting glycemia, gestational diabetes in previous pregnancies); glucosuria during pregnancy (the appearance of glucose in the urine).
Gestational diabetes mellitus, which first developed during pregnancy, often does not have clinical manifestations associated with hyperglycemia (dry mouth, thirst, increased volume of urine excreted per day, itching, etc.) and requires active detection (screening) during pregnancy !
Gestation
Gestation is, in fact, the definition of the term pregnancy, with the difference that the gestation period is determined by the number of full weeks of the period when a pregnant woman is carrying a child. The beginning of gestation is calculated from the calendar date from the beginning of the last menstrual cycle, before the onset of the observed pregnancy, and ends with the moment the woman gives birth, or, in more dire options, with an induced abortion or spontaneous miscarriage. If it is not possible to establish correct data on menstruation, then the gestational age of pregnancy can be determined by an obstetrician-gynecologist using other studies, clinically detectable signs and, directly, the method of ultrasound examination.
The beginning of gestation is important to determine by the leading doctor of the antenatal clinic, not only to determine the approximate life span of the fetus, but also to most accurately calculate the date of birth. This point is very significant for the girl who is carrying a child, since she will know the expected time and will have the additional opportunity to think through everything in advance and prepare for the birth of the child.
It is generally accepted that, according to the gestational age assigned, newborn children are divided into the following categories: premature, born within the given period of time are full-term, or those born beyond the given period are post-term.
It is also important to distinguish the obstetric period from the gestational period, which can often not be differentiated, although they differ by approximately a two-week interval.
Gestation - what is it?
Gestational age is a generally accepted term used to more accurately determine the timing at which the child will be in the womb of its mother. When determining the timing of menstruation, there is a risk of a slight error in determining the onset of the gestational period, and all because the very moment of the origin of fertilization is extremely difficult to find out.
The physiology of gestation is that in order for life to arise, or rather its debut in the correct way, it would be worth counting from the fertilization of a mature egg and the moment of implantation of the egg with the fetus. But, in fact, after sexual intercourse, it takes up to several days for a particular sperm to reach its goal and the birth of a completely new life to take place, and also for the fertilized egg to travel its way from the fallopian tubes to the uterus itself and then become entrenched in its wall. Actually, this is why doctors believe that the gestational age is inaccurate and unreliable, using the “obstetric term” for setting the gestational age.
The “obstetric method” is more accurate than the gestational age, but it is ahead of it, since the countdown comes not from the first, but from the last calculated day of the last menstruation, because ovulation itself occurs in the middle of this cycle, and without it, fertilization, as such, is actually impossible. Obstetricians-gynecologists determine the gestational age only once, namely, after conducting an examination with an ultrasound sensor, during the first examination at about 8-12 weeks of pregnancy, when diagnosing pregnancy, and when registering a woman in a female outpatient department consultation overnight.
After the ultrasound, the doctor calculates gestation using a specially created formula:
W = 13.9646 KTE – 4.1993 + 2.155
Where W is the gestational indicator, KTP is the coccygeal-parietal value. A similar calculation is carried out throughout the first ninety days of pregnancy, that is, the first three months of gestation. And starting from the fourth gestational month, doctors opt for using a different indicator of values. This indicator is as follows: the coccygeal-parietal value is measured by the biparietal size of the fetal head, and the determination of gestational age is calculated according to the following formula:
W = 52.687-0.67810.011-76.7756 x H
where B is the biparietal size of the head (indicated in units of millimeters).
The gestational age is important for the attending physician to understand in order to pre-calculate the main expected date of the birth itself. The very date of birth is found out in order to determine whether in the future the baby born will be born at the generally accepted time, or may be premature or post-term. Since in this scenario, which is dangerously threatening to the life of a newborn baby and serious health consequences may arise for both the mother and the baby, it will be necessary to prepare or redirect to specialized perinatal centers.
A full-term baby is one born between 37 and 42 weeks (in the period of days between 260–294). Premature births are considered to be those that occurred before the 38th week of gestation; this option threatens the underdevelopment of the organ systems of the fetus at birth (for example, immaturity of nervous structures, respiratory characteristics - immaturity of surfactant, lungs do not expand for the first breath).
In the case of transition with labor, that is, childbirth after the forties, or more precisely 41–42 weeks of pregnancy, this threatens the possibility of infection in utero if the amniotic fluid is contaminated (impaired sterility), the developed large fetus during the process of passing through the birth canal can injure the mother’s body and hurt yourself too.
Completion of gestation is the period that follows the end of childbirth.
Degrees of gestation
The degree of gestation, which is actually the age of the embryo and fetus in the mother’s womb from the time of fertilization, corresponds to the gestational age in the modern classification, this degree is correlated with the degrees of full term of children and prematurity, and according to previously accepted degrees of gestational age, they are divided into the following subtypes:
- The first degree of gestation, which corresponds to 37-35 weeks of gestation and often such babies are born with a preliminary weight of 2500-2001 grams and their height reaches 45-41 cm.
- Second degree of gestation, which corresponds to 34-32 weeks of gestational age and with an estimated weight of 2000-1501 grams and a body length of about 40-36 cm.
- Third degree of gestation, with a time limit of 31-29 weeks and a weight in the range of 1500-1001 grams and 35-30 cm of height.
- And the last, fourth degree of gestation with a borderline value of up to a weekly gestational value of 29, and a borderline weight of the born baby of 1000 or less, a length of less than 30 cm. They are also called the term “premature babies with extremely low weight.”
Today, the degrees of gestation still fade into the background, and in the modern medical community it is customary to formulate a diagnosis of gestation according to instrumental indicators and the baby’s weight at birth. The borderline weight in such observed newborns has a margin of error for weight loss of up to 12% by the newborn week; recovery occurs significantly late in comparison with full-term ones, approximately by the end of the newborn period, that is, by the 28th day of the child.
The fact of prematurity, with proper care, does not have a particularly strong impact on the development of the child. By the age of two or three, such children catch up with their same-year-old peers, both in all standard indicators, and quite possibly even surpass them, but provided that they have been involved with the children and given them due attention and care.
According to different degrees of gestation, the approach to such children is also different. They are nursed either at home (with mild prematurity) or in conditions specially created for them, in several successive stages (deep prematurity). Thus, in children with an initial weight of over 2300 grams, this complex is limited to special procedures and upon discharge the weight is already sufficiently normalized for home monitoring. When born with a lower weight, discharge may take up to three to four months, since nursing and recovery of such babies is more labor-intensive and takes three stages: 1) maternity hospital; 2) a specialized department of the hospital; 3) home care.
Gestational age - how to calculate?
The gestational age is calculated in several ways, they are as follows:
- The first method, in which it is necessary to know exactly the date of the beginning of extreme menstruation, as well as the regularity and duration of the menstrual cycle itself, and whether there are any disruptions in its passage. And age is calculated from the first day, and not from the moment of conception.
— The second method, namely ultrasound examination at the earliest stage, is currently considered the most informative and indicative for determining the gestation of the fetus during pregnancy. This method is especially good because to use it it is not necessary to know the timing of menstruation, which women often forget; determining the moment of conception is also not very easy, but by resorting to this method it is possible to clarify all this. And this study can be carried out already at the very initial stages of pregnancy, starting almost from the fifth week of gestation, but still the more recommended period is from the eighth to the eighteenth week. An ultrasound vaginal sensor allows you to determine the size of the embryo or fetus, the rate of development, the presence of pathologies, and allows you to directly determine which gestational week is at the time of the study.
- The third way. Obstetricians-gynecologists determine the gestational age only once, namely, after conducting an examination with an ultrasound sensor, during the first examination at about 8-12 weeks of pregnancy, when diagnosing pregnancy, and when registering with a polyclinic department - antenatal clinic. department, overnight.
After the ultrasound, the doctor calculates gestation using a specially created formula:
W = 13.9646 KTE – 4.1993 + 2.155
Where W is the gestational indicator, KTP is the coccygeal-parietal value. A similar calculation is carried out throughout the first ninety days of pregnancy, that is, the first three gestational months. And starting from the fourth gestational month, doctors opt for using a different indicator of values. This indicator is as follows: the coccygeal-parietal value is measured for the biparietal size of the fetal head, and the determination of gestational age is calculated according to the following formula:
W = 52.687-0.67810.011-76.7756 x H
where B is the biparietal size of the head (indicated in units of millimeters).
The gestational age of a child can most accurately and correctly be established on the basis of a synchronous definition and integral characteristics of several neurological and morphological signs of the child’s maturity according to the so-called Dubovich scale.
What is gestational dominance?
The term “gestational dominant” is quite often found in the results of studies in pregnant women. In itself, this diagnosis means that during the gestation period, such a pregnant woman had negative factors influenced by external environmental indicators, namely, the woman experienced both physiological changes in the body and psycho-emotional ones. The latter triumph over the awareness of oneself and the world around it and manifest themselves in the following: nervousness, excessive tearfulness, increased vulnerability, sudden behavioral changes and mood disorders, depressive moments, even suicidal thoughts.
All this is very fraught with the fact that the future woman in labor begins to have incorrect thoughts, regarding psychoneurological aspects and the public, that the fault of her poor condition is pregnancy, they see in her the “root of evil”, considering this condition as a pathological change and it spoils her normal and habitual life. life, violating her “comfort zone”, the very fact of bearing a child is perceived as a psychotraumatic factor. This has an extremely negative and deplorable effect on the mother in the future: dislike or even hatred of the baby, postpartum depression, suicidal tendencies, refusal of maternal responsibilities, reluctance to breastfeed, approach the baby, and the like. All these mental pathologies and changes lead to severe and serious psychoneurological problems in such a woman.
Necessary tests
All pregnant women must have their fasting venous blood plasma glucose tested in a laboratory (cannot be tested using portable glucose self-monitoring devices - glucometers!) - against the background of a normal diet and physical activity - upon first contact with the antenatal clinic or perinatal center (as possible earlier!), but no later than 24 weeks of pregnancy. It should be remembered that during pregnancy the blood glucose level on an empty stomach is lower, and after eating it is higher than outside pregnancy!
Pregnant women whose blood glucose levels, according to WHO recommendations, meet the diagnostic criteria for diabetes mellitus or impaired glucose tolerance are diagnosed with gestational diabetes mellitus. If the results of the study correspond to normal indicators during pregnancy, then an oral glucose tolerance test - OGTT ("stress test" with 75 g of glucose) is mandatory at 24-28 weeks of pregnancy in order to actively identify possible disorders of carbohydrate metabolism. All over the world, OGTT with 75 g of glucose is a safe and the only diagnostic test for detecting disorders of carbohydrate metabolism during pregnancy!
| Research time | Venous plasma glucose | ||
| On an empty stomach | > 7.0 mmol/l (> 126 mg/dl) | > 5.1 < 7.0 mmol/l (>92<126 mg/dl) | <5.1 mmol/L (<92 mg/dL) |
| At any time of the day if there are symptoms of hyperglycemia (dry mouth, thirst, increased volume of urine excreted per day, itching, etc.) | > 11.1 mmol/l | — | — |
| Glycated hemoglobin (HbA1C) | > 6,5% | — | — |
| OGTT with 75 g anhydrous glucose h/w 1 hour after meals | — | >10 mmol/l (>180 mg/dl) | < 10 mmol/l (<180 mg/dl) |
| OGTT with 75 g anhydrous glucose h/w 2 hours after meals | — | > 8.5 mmol/l (> 153 mg/dl) | <8.5 mmol/l (<153 mg/dl) |
| Diagnosis | diabetes mellitus type 1 or 2 during pregnancy | Gestational diabetes mellitus | Physiological blood glucose levels during pregnancy |
Remember that normalizing carbohydrate metabolism in a pregnant woman allows you to avoid complications from both the course of pregnancy itself and the condition of the fetus!
After a diagnosis of gestational diabetes mellitus is made, all women require constant monitoring by an endocrinologist together with an obstetrician-gynecologist. Pregnant women should be trained in the principles of rational nutrition, self-control and behavior in conditions of a new pathological condition (i.e., timely testing and visits to specialists - at least once every 2 weeks).
A pregnant woman's diet should be sufficiently high in calories and balanced in basic food ingredients to provide the developing fetus with all the necessary nutrients. At the same time, in women with gestational diabetes mellitus, taking into account the characteristics of the pathological condition, nutrition should be adjusted. The basic principles of diet therapy include ensuring stable normoglycemia (maintaining blood glucose levels corresponding to those for physiological pregnancy), and preventing ketonemia (the appearance of fat breakdown products - “hungry” ketones - in the urine), as mentioned above in the text.
Increased postprandial blood glucose levels (above 6.7 mmol/L) are associated with an increased incidence of fetal macrosomia. Therefore, a pregnant woman should exclude easily digestible carbohydrates from food (which lead to a rapid uncontrollable rise in blood glucose) and give preference in the diet to difficult-to-digest carbohydrates high in dietary fiber - carbohydrates protected by dietary fiber (for example, many vegetables, legumes) have a low glycemic index. The glycemic index (GI) is a factor in the rate of absorption of carbohydrates.
Gestational age: what is it and how to calculate it?
Gestational age is a term that defines the length of time a baby spends in the womb from conception to birth. Doctors usually start reporting from the last day of your last period. This is due to the fact that the moment of fertilization itself is very difficult to recognize.
How to calculate the deadline correctly?
The gestational age of pregnancy is the very moment when a new life is born in a woman. But, unfortunately, not all couples know exactly when the egg was fertilized and when the egg was implanted with the fetus. After sexual intercourse, it takes several days for the sperm to reach its goal and the birth of a new life to occur, as well as for the egg to travel to the uterus and become established in it. This is why doctors consider the gestational age unreliable.
Gynecologists and obstetricians have their own method for determining the age of the baby in the womb, it is called the “obstetric method”. They believe that it is more accurate than the gestational age, but is about a couple of weeks ahead of it, because it is calculated from the last day of the last menstruation, and ovulation occurs only in the middle of the cycle. Without ovulation, fertilization is impossible.
Doctors and obstetricians most often determine the gestational age only once; after an ultrasound, they recalculate it using a special formula:
Ш = ? 13.9646KTR – 4.1993 + 2.155
Here W is a gestational indicator, and KTR is the parietal-coccygeal size. This calculation is carried out during the first 90 days of pregnancy.
From the fourth month, doctors prefer to use a different value. They replace KTR with BPR (fetal head size is biparietal).
Gestational age is determined using the formula:
W=52.687-0.6?7810.011-76.7756 x H
In this case, B is BPR (measured in millimeters).
Why is timing important?
Gynecologists seek to find out the gestational age of the fetus in order to preliminarily calculate the estimated date of birth (ED). This is necessary in order to exclude prematurity and postmaturity of the baby. After all, both of these conditions are dangerous for the child, because they can have serious consequences for the health of the mother and baby. Premature birth occurs before the 38th week of pregnancy and it threatens the underdevelopment of the fetus at birth, the baby’s lungs may not expand, etc. When nursing, labor can begin after 41–42 weeks of pregnancy and threatens to infect the child due to contamination of the amniotic fluid; the child, due to its large size, can have difficulty moving through the birth canal, thereby injuring the mother or himself.
Completion of gestational age
According to people who are far from even the basics of gynecology, the gestational age and the estimated date of birth are one and the same. But this is absolutely not true. A woman will not start giving birth just because she has PDD today. It depends on the baby, on his readiness to be born and on how ready the pregnant woman’s body is. Doctors consider the end of the gestational period to be that which occurs after the end of childbirth.
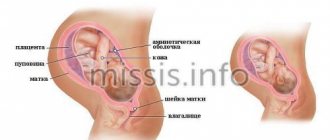
In the photograph you can see how the body of a pregnant woman changes as the gestational age increases.
What other methods are used to set a deadline?
Sometimes it happens that the gestational and obstetric dates cannot be calculated. This happens when pregnancy occurs after childbirth or while breastfeeding, the woman does not have a regular menstrual cycle or there are hormonal imbalances. During these periods, representatives of the fairer sex do not have periods, but there is an opportunity to become pregnant. In such situations, gynecologists prescribe an ultrasound scan (ultrasound diagnostics). Thanks to this device, you can accurately determine the presence of pregnancy and the exact duration of pregnancy. The most suitable period for examination is considered to be 7–17 weeks. The gestational age is determined by the size of the child.
No matter how accurate all three methods of determination are, the estimated date of birth may differ.
Many girls who are pregnant for the first time wonder: what does gestational age mean? And this means the age of the fetus. Doctors use their own methods to determine it in order to preliminarily calculate the estimated date of birth. This is necessary in order to exclude premature birth and nursing.