Intestinal obstruction is a complex of symptoms that develop against the background of a complete or partial disruption of the movement of food through the intestines. Intestinal obstruction is a dangerous condition, which, if left untreated, is inevitably complicated by peritonitis, intestinal necrosis and leads to the death of the patient. Therefore, you need to start treating this disease as early as possible.
- Causes and types of acute intestinal obstruction
- Consequences of intestinal obstruction
- Symptoms of intestinal obstruction
- Diagnosis of intestinal obstruction
- Treatment of intestinal obstruction and first aid
Causes and types of acute intestinal obstruction
Depending on what caused its development, there are:
- Dynamic or functional obstruction. It develops due to a violation of intestinal motility - its spasm or paralysis.
- Mechanical intestinal obstruction. It develops due to the closure of the intestinal lumen and the impossibility of transit of its contents. Here they distinguish:
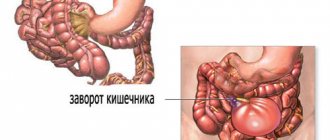
- Strangulated intestinal obstruction, from the Latin strangulatio - strangulation. It develops due to compression of the intestine or its mesentery, as a result of which the blood supply to the intestine is disrupted. This is a very dangerous condition as it can lead to necrosis of the intestinal wall.
- Obstructive intestinal obstruction. Develops due to blockage (obstruction) of the intestinal lumen by foreign bodies (calculi, parasites), tumor or scar deformation.
Depending on the site of development, colonic and small intestinal obstruction are distinguished.
In oncology, intestinal obstruction most often has an obstructive nature and develops as a complication of colorectal cancer, when the tumor blocks the lumen of the colon, usually in its terminal stages. Obstruction can also develop as a result of compression of the intestine by a tumor of another organ, for example, the uterus or prostate gland.
Small intestinal obstruction occurs less frequently. As a rule, its cause is carcinomatosis of the visceral peritoneum. Primary tumors in this region are extremely rare.
Preoperative testing
If you have symptoms of a bowel obstruction, your doctor will do a physical exam to check your stomach and bowel sounds.
Diagnostic evaluation may include an abdominal x-ray, computed tomography (ultrasound) scan, or ultrasound. These tests may or may not include a barium enema, which involves injecting a small amount of contrast material into the rectum to better visualize the structures.
If you have a blockage, you may also need a sigmoidoscopy or colonoscopy, which are invasive diagnostic procedures in which a camera is inserted into the colon to visualize the blockage.
Consequences of intestinal obstruction
The development of obstruction triggers a cascade of pathological processes that affect the body systemically. With tumor obturation, the onset, as a rule, is blurred due to incomplete occlusion of the intestinal lumen, but as the tumor grows, the situation worsens. Acute obstruction, as a rule, develops due to complete obstruction of dense feces in the area of the intestine narrowed by the tumor.
In the first time after the development of obstruction, there is an increase in intestinal peristalsis. It's as if he wants to overcome an obstacle. As intestinal contents accumulate, the intestinal wall becomes overstretched, water-electrolyte and metabolic disturbances occur, motor function sharply weakens, and then intestinal paralysis occurs.
At the second stage, disturbances in the secretory-resorptive activity of the intestine and disturbances in parietal digestion develop, the enzymatic activity of enterocytes is blocked, as they are rejected, and the regenerative activity of the crypts is first inhibited and then completely stopped.
Under such conditions, the activity of intestinal bacteria and the so-called symbiont digestion is activated. It is not physiological and is inferior in efficiency to normal, parietal digestion. As a result, rotting and fermentation occurs, as well as the accumulation of a large number of products of incomplete breakdown of proteins, some of which have a toxic effect.
As the process progresses, the immune defense mechanisms are disrupted, which leads to the active proliferation of anaerobic bacteria that secrete exo- and endotoxins. They act systemically on the body - they disrupt tissue microcirculation, lead to central nervous system disorder, and disrupt cellular metabolism. Due to these effects, the permeability of the intestinal wall to bacteria increases, and they can spread into the abdominal cavity, blood and lymph flow, causing peritonitis and even sepsis.
Water and electrolyte disturbances also progress. Due to disruption of the intestine, increased filtration of fluid occurs; it is not absorbed back and accumulates in the afferent loop of the intestine. Under normal conditions, about 10 liters of liquid enter the gastrointestinal tract per day (including food, drink, saliva and secretions of the digestive glands). About 8-9 liters should be absorbed back, but this does not happen due to impaired reabsorption. Fluid accumulates in the adductor section of the intestine, causing it to expand. This, in turn, leads to reflex vomiting, which further worsens dehydration. Against this background, electrolyte disturbances quickly develop, which ultimately lead to renal and heart failure.
Book a consultation 24 hours a day
+7+7+78
Symptoms of intestinal obstruction
- Pain. This is one of the very first signs of intestinal obstruction. It is observed in absolutely all patients. With tumor obstruction, pain occurs suddenly, for no apparent reason, and may even be one of the first signs of cancer. It has a cramping character. The greatest pain occurs at the time of peristaltic contractions, after which it subsides a little for a couple of minutes. Gradually, the intensity of the pain increases and after a few hours it becomes unbearable. They subside only on the 2-3rd day, when paralysis of the intestine already develops - “noise at the beginning, silence at the end”, a symptom of “grave silence”, when there are no sounds of peristalsis at all.
- Vomit. If the obstruction is located at the level of the small intestine or the right part of the large intestine, vomiting will be present in the early stages, as a sign of reflex irritation of the gastrointestinal tract. If there is obstruction of the terminal sections, vomiting will most likely not occur at first, or it will occur at large intervals. During breaks, patients may suffer from nausea, hiccups or belching. If intestinal obstruction persists, vomiting becomes indomitable, first the stagnant contents of the stomach and then the intestines are released, up to vomiting of feces. This is a bad sign, because it indicates that vomiting is a symptom of toxic cerebral edema, and it cannot be eliminated by draining the gastrointestinal tract.
- Retention of stool. This symptom is observed with obstruction at the level of the sigmoid and rectum. If there is high obstruction at first, the stool may persist.
- Bloating. There are 4 signs here: asymmetry of the abdomen, palpable bulge of the intestine, peristaltic contractions of the intestine that can be seen with the naked eye, tympanic sound upon percussion.
- Bloody or mucous discharge from the rectum. They usually occur with cancer of the terminal sections of the intestine and are associated with the secretion of mucus by the tumor, its disintegration, or injury from feces.
In the process of developing the clinical picture of intestinal obstruction, three periods are distinguished:
- Early – up to 12 o’clock. The main symptom of this period is cramping swelling in the abdomen. Vomiting develops rarely and only with obstruction (blockage) at the level of the small intestine.
- The intermediate period is from 12 hours to a day. At this time, the symptoms continue to increase and turn into a detailed picture. The pain becomes intense and even unbearable, without contractions, an enlarged abdomen, vomiting, and signs of dehydration appear.
- Late period – more than 24 hours. The patient's condition worsens, the temperature rises, and a systemic inflammatory response develops, including peritonitis and sepsis. Shortness of breath and heart failure worsen.
Benefits of treatment at GMS Hospital
GMS Hospital is a multidisciplinary medical center. Every year more and more patients trust us with their health and there are reasons for this:
- Our clinic has the opportunity to carry out the necessary diagnostic tests as soon as possible and, if the diagnosis is confirmed, to carry out immediate treatment. It is for the convenience of our clients that the emergency surgery department operates around the clock.
- Doctors at GMS Hospital are specialists with many years of experience who are proficient in modern operational techniques for performing emergency operations.
- An integrated approach to patient treatment - consultation and supervision of specialists in related specialties at all stages of your stay in the clinic.
- Modern treatment, advanced technologies, high-class medical equipment to minimize the risk of postoperative complications.
- The interest of medical personnel in the speedy recovery of the patient.
Diagnosis of intestinal obstruction
The diagnosis of intestinal obstruction can be suspected based on the patient’s characteristic complaints. Confirmation is made using instrumental examination.
The simplest, fastest and most accessible diagnostic method is a survey radiography of the abdominal organs. The photographs reveal characteristic features:
- Kloiber's cup - dilated intestinal loops in the form of domes are visible, and there is a horizontal level of liquid in them. This painting resembles a bowl turned upside down. There may be several bowls; in the picture they are layered on top of each other.
- Intestinal arcades - arise due to swelling of the loops of the small intestine with gases; a horizontal level of fluid is visualized in the lower knees of the intestine.
- Kerking's folds - due to stretching of the jejunum on radiographs, it takes on the appearance of an extended spring.
- X-ray studies with contrast can also be used, for example, a study of the passage of barium suspension through the gastrointestinal tract, or irrigoscopy. However, these methods take a lot of time and delay the decision on the need for surgery.
Other diagnostic methods used:
- Endoscopic examination, such as colonoscopy or sigmoidoscopy. Such a study helps determine the localization of the tumor and the level of stenosis in the obstructed intestinal segment. In some cases, it is possible to pass a probe through the stenotic area and drain the afferent intestine. Colonoscopy is not performed if the patient’s condition is severe, there are symptoms of peritonitis and there is a risk of tumor perforation.
- CT. Using this study, it is possible to visualize the tumor, its size and the extent of stenosis (narrowing). In addition, the relationship of the cancer with surrounding tissues can be assessed and the presence of metastases can be determined.
- Ultrasound. In case of obstruction, an increase in the intestinal lumen, accumulation of air (gases) in it, and thickening of the intestinal wall due to inflammation are visualized. With the development of systemic inflammatory processes, free fluid may be detected in the abdominal cavity.
Patients with contraindications to surgery - is it possible to help?
As for weakened patients, in cancer patients with severe exhaustion, the absence of stool for a couple of days is acceptable. All other patients, including those with neurological pathologies, for example, those suffering from Alzheimer's or Parkinson's disease, require urgent hospitalization; in case of intestinal obstruction, such patients should be under constant medical supervision. In this situation, surgery is prescribed as a last resort - if it was not possible to alleviate the patient’s condition within 2-3 days, as well as if there is a risk of developing coprostasis. If surgery is contraindicated, then colon stenting using endoscopic equipment is possible as palliative treatment. All manipulations are carried out through a natural opening: a balloon is inserted into the intestinal lumen, expanding the narrowed section of the intestine, after which a stent is installed. In this way, it is possible to avoid or postpone abdominal surgery in an inoperable patient, improving his quality of life.
Intestinal obstruction is a dangerous condition, the outcome of which depends on timely medical care. But complete recovery, even in severe cases, is possible if the patient is urgently hospitalized in the surgical department. Therefore, when the first symptoms appear, contact us immediately - this way you can avoid serious consequences, or even save your life; everything depends on you!