Multiple sclerosis is a fairly common diagnosis nowadays and, importantly, it is given to young and middle-aged people (15–40 years old). MS is a disorder of the nervous system caused by:
- genetic predisposition (gene mutation);
- infections and viruses of various kinds;
- lack of vitamins, especially group D;
- injuries;
- malfunctions of the immune system;
- severe stressful situations, etc.
Also at risk are diabetics and people with thyroid and intestinal diseases.
In Russia, about 40 people per 100,000 population have this disease, in other countries this ratio is up to 200 per 100,000 population. Women are diagnosed three times more often than men. The phenotype of the disease is fair-haired European women. If the diagnosis is not made on time, this can lead to serious complications, including disability. That is why you need to pay attention to the symptoms of the disease in time.
Symptoms of multiple sclerosis in women
The disease's manifestations are vague and mimic many other neurological conditions. The clinical picture of MS is very diverse, depending on the shape, course and location of the lesion. It happens that a woman has only one symptom. More often - several.
- Movement disorders. What most often begins with multiple sclerosis. Motor disorders include paresis and paralysis. Paresis is an incomplete impairment of voluntary movement of the limbs. Paralysis is a complete impairment, without the ability to voluntarily move the limbs. This pathology is the main reason for the transformation of patients into disabled people.
- Sensitivity disorders. So-called paresthesia is a burning sensation, tingling in the limbs, comparable to goosebumps or muscle spasm. Other types of sensitivity are also impaired: vibration, joint-muscular, temperature. Sensitivity may decrease or disappear completely.
- Pathology of vision. Occurs due to changes in the optic nerve. Possible manifestations:
- decreased visual acuity;
- the appearance of a blind area of the visual field - scotoma;
- nystagmus - rapid uncontrolled movements of the eyeballs;
- incorrect color perception.
- in the lower extremities;
- in the pelvic area;
- headache;
- muscle and joint pain;
- pain on one side of the face (trigeminal neuralgia).
The very first changes can only be noticed by a neurologist during a clinical examination.
Expert opinion
Author: Alexey Vladimirovich Vasiliev
Neurologist, Head of the Research Center for Motor Neuron Disease/ALS, Candidate of Medical Sciences
Multiple sclerosis is an autoimmune demyelinating disease. According to the World Health Organization, the number of people with this diagnosis has exceeded two million, with 2-3 times more women (researchers give different figures), but in men the disease is more severe.
The autoimmune nature indicates that the cause of the disease is inside the person, or more precisely, the immune cells attack the “wrong” target, in this case, the myelin sheath of the neuron, which is why the “signal disappears.” But why women? The fact is that when a woman is carrying a child, her immune system perceives this as a threat and its functioning may be disrupted.
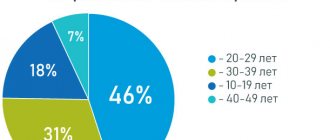
Multiple sclerosis is not a disease of older people. The average age of onset of relapsing-remitting forms is 30 years, with women acquiring the disease earlier. 5% of MS cases are children under 18 years of age and approximately 10% are patients over 50.
Multiple sclerosis cannot be cured; therapy is aimed at relieving symptoms. With early detection and adequate treatment, the prognosis is good, but experts say that MS shortens life expectancy by 7-14 years.
How to understand that you are sick?
The initial stage of multiple sclerosis is characterized by alternating relapses (attacks, exacerbations) and remissions. MS in most cases (75-85%) begins in a remitting form. Common symptoms of early-stage multiple sclerosis do not differ between women and men and include:
- sensitivity disorders;
- movement coordination disorder;
- ocular movement disorders (nystagmus);
- sexual and sphincter dysfunctions;
- inflammation of the optic nerve is often present.
In most cases, early stage symptoms subside within 6-8 weeks, but can sometimes leave a permanent abnormal neurological finding or some degree of disability. The ability to reverse the effects of multiple sclerosis in women usually decreases as the disease progresses. The periods of alternating attacks and remission last about 5-15 years. Inflammatory activity on MRI at this stage is the highest.
- MS is a complex disease. It takes about 7 years from the onset of the first symptoms in women in the early stages to the diagnosis of multiple sclerosis. So what should you focus on? What signs are a reason to see a doctor? Changes in sensation in the limbs: tingling, trembling, numbness in the legs;
- sensations resembling an electric shock, moving along the spine or radiating to the limbs.
Dizziness in MS has an uncharacteristic course and is often accompanied by loss of limbs and pins and needles throughout the body. What is multiple sclerosis like and how to live with it, how the first symptoms appear - a woman’s view of the problem from the inside:
Forms of female MS
Depending on the location of the lesion, the following forms of MS are distinguished:
- Cerebral. Manifested by impaired brain function and epileptic seizures.
- Stem. The fastest form of the onset and development of the disease, the patient often does not even have time to assess the situation.
- Optical. Visual impairment.
- Spinal. Spinal cord dysfunction.
- Cerebrospinal. Several body systems are affected at once. The most common form of MS.
- Cerebellar. It is characterized by damage to the cerebellum, which leads to impaired movements and hand tremors.
Make an appointment
Cerebral form
Characteristic in case of damage to the motor area (responsible for movement) of the brain. Changes in the cells of the central part of the brain lead to paralysis and paresis (decreased muscle strength) of various forms. If limbs on one side are involved in this process (for example, the right arm and leg), we can talk about hemiparesis; two limbs (for example, two arms or two legs) - about paraparesis; all four limbs (2 arms, 2 legs) - tetraparesis.
Stem form
It is localized in the brain stem - the place responsible for all our sensitivity in general. Violations here most often lead to problems with speech (it is impossible to pronounce words clearly, the tone and timbre of the voice changes) and breathing (the muscles in the larynx relax so that they block the access of air to the trachea). This form has a lightning-fast course: a person begins to choke, the temperature rises sharply and an unbearable headache appears. Only immediate resuscitation can help here, but death often occurs.
Optical form
MS in this case is localized in the occipital lobe of the brain, which is responsible for vision. The course of the disease in this case is usually as follows: first, the colors become duller, then visual acuity decreases, then vision deteriorates until complete blindness. The lesion can affect one or both eyes at once. If the disease is relapsing-remitting, vision may return to its previous state even without treatment.
Other symptoms may also occur: double vision, pain, inability to look to the side, eye twitching, etc.
Spinal shape
The source of the disease in this case is located in the spinal cord. Manifestations of this form of the disease are usually as follows:
- lower paraparesis (muscle weakness in both legs);
- decreased sensitivity;
- “shooting” in the arms and legs (Lhermitte syndrome);
- disruption of the functioning of the genitourinary system.
Cerebrospinal form
The most common form of MS. It affects both the brain and spinal cord simultaneously, and therefore the visual and vestibular apparatus. This form combines the symptoms of cerebral and spinal forms.
Cerebellar form
The location of the lesion is the cerebellum, which is responsible for the coordination of movements. Accordingly, the symptoms of this form will be as follows:
- impaired coordination of movements;
- inability to adequately estimate the distance to an object;
- trembling in the limbs;
- loss of the ability to move at all;
- severe headaches;
- impossibility of articulate pronunciation due to limited mobility of the speech organs (lips, tongue, soft palate).
Symptoms of the leak
Symptoms of multiple sclerosis in women vary depending on which part of the spinal cord or brain is affected. In addition, symptoms may appear or disappear, which complicates the diagnosis of the organism. Frequent signs of the development of early multiple sclerosis are:
- severe weakness in the limbs;
- constant fatigue of the body with minor loads;
- a sharp deterioration in a person’s visual functions with rapid recovery;
- numbness of the limbs;
- headache;
- dizziness;
- severe incoordination of movement;
- men may develop impotence;
- epilepsy appears.
If left untreated, these symptoms intensify, leading to:
- vision;
- speech patterns;
- swallowing problems appear;
- dry mouth;
- lack of sleep and desire to eat;
- severe decrease in mental abilities;
- urinary and fecal incontinence;
- dementia develops.
Only timely treatment and early diagnosis of this pathology can save a person from rapid disability and delay its onset.
Types of PC
According to the clinical course, experts distinguish the following forms of MS:
- Relapsing-remitting form (RRMS). Secondary progressive form. It is characterized by rather pronounced manifestations. Exacerbations in this case are rare (or generally unnoticeable against the background of constant symptoms), but residual signs of multiple sclerosis are present during stabilization. 30–40% of patients are in this group.
- Primary progressive form (PPMS). The disease is constantly progressing, periods of improvement are insignificant. Exacerbations are not clearly identified. 10–15% of patients belong to this group. A striking example is when a patient’s vision begins to decline and is no longer restored (even for a short time), but only worsens.
- Secondary progressive course (SPRS). It is characterized by a slow deterioration of the condition, the occurrence of complications over a long period of time. This form of MS can be either active (with attacks) or not. Usually occurs after RRMS. Selective damage occurs to the myelin sheath that runs around the nerve fibers of the central nervous system.
- Progressive course with exacerbations. The disease is constantly progressing, with exacerbations occurring as MS develops. After each exacerbation, the patient's condition worsens. 5% of patients fall into this group.
To determine which group according to the course of the disease the patient belongs to, specialists prescribe a series of examinations.
Make an appointment
Relapsing-remitting form
As mentioned above, relapses in this form alternate with remission, during which no progression of the disease is observed.
To diagnose RRMS, a specialist needs to detect the spread of the disease in at least two areas of the central nervous system (affected areas of myelin, the substance that forms the sheath of nerve fibers). An important criterion here is the prevalence over time, that is, damage to these areas should occur at different times. If one of the criteria is not confirmed, a clinically isolated syndrome can be diagnosed with further clarification of the diagnosis.
With this form of the disease, patients usually experience the following symptoms:
- fatigue;
- numbness of the limbs;
- loss of vision;
- memory problems;
- disturbances in the functioning of the genitourinary system.
At the same time, people with progressive forms of MS are more likely to have problems related to the musculoskeletal system.
Primary progressive
This course of the disease is accompanied by sharp deterioration without early relapses and remissions. This form of MS is more difficult to diagnose. On average, PPMS occurs several years (about 8–10) after a relapsing-remitting course. Since in this course of MS the spinal cord is more often affected than the central nervous system, the patients’ problems are usually associated with walking, urinary and fecal incontinence.
Secondary progressive
This form can only be diagnosed in a patient already diagnosed with multiple sclerosis. To understand whether the transition from RRMS to SPMS has taken place, it is necessary to be constantly monitored by a neurologist and periodically do MRI. Due to the appearance of new foci in this course, exacerbations and relapses are possible, as with RRMS. The nature of the disease slowly moves from the demyelinating stage to the neurodegenerative stage, characterized by damage to nerve fibers and tissues.
Progressive with exacerbations
The rarest form in which the disease, starting with a remitting course, becomes primary progressive. In this case, symptoms increase, and neurological functions do not recover after exacerbations.
Some notes on the course of the disease in women
Primary signs of multiple sclerosis in women are most often not detected, even when the patient has already developed MS plaques in the brain; the onset may go unnoticed, or it may immediately cause enormous damage to health; the disease can manifest itself in different forms.
Approximate options for recognizing the onset of the disease:
- due to weakened vision, sensory impairment;
- the pathology did not manifest itself in any way, but by chance an MRI study showed focal brain damage.
The mechanism of pathology development includes the process of compensation by intact nerve fibers for damage to a small amount of nervous tissue. Until the damage is 40 - 50%, focal neurological signs do not manifest themselves.
The typical course of the disease in women occurs with alternating moments of exacerbation and remission, in men there is a relentless intensification of the disease
. It is believed that female hormones block the dynamics of the development of astrogliosis and the nerve cell membrane is able to recover.
There is no classification of specific signs of multiple sclerosis for different patients. They are individual for each patient. The disease can reveal itself by one or a group of signs depending on the location of the foci of demyelination
.
Causes
As we said above, women are more susceptible to this disease than men. But, interestingly, their immune system resists MS better than men’s.
Until now, the nature of MS remains a mystery. However, thanks to laboratory and clinical studies, the mechanism of MS development is known. Based on this, the most important factors were identified:
- Infections. There is no single infectious disease that leads to MS. However, some infectious agents cause specific autoimmune reactions that may be responsible for multiple sclerosis. Among them:
- herpes virus;
- endogenous retroviruses;
- Epstein-Barr virus;
- various bacterial infections.
Prevention of sclerosis
Prevention of multiple sclerosis includes:
- Cigarettes and alcohol accelerate the destruction of neurons and can cause damage to the immune system.
- Monitoring your weight, avoiding strict diets and overeating.
- Avoidance of hormonal medications (if possible) and contraceptives.
- Refusal of large amounts of fatty foods;
- Avoid overheating. Alzheimer's disease - what it is, symptoms and signs, causes, treatment, stages.
Multiple sclerosis is an incurable disease that can lead to disability, but this is not a death sentence. It is important to diagnose the disease in time and follow all doctor’s instructions. Then a person has a chance to live to an old age and maintain good spirits. Primary prevention (directly aimed at preventing the disease) does not exist. You can protect yourself a little from multiple sclerosis or its relapses if you exclude any infections, stress, injuries, surgeries, and smoking.
Diagnostics
MS is a disease in which the timing of diagnosis plays a critical role. The earlier the disease is detected, the greater the patient's chances for a normal life. Neurologists first collect anamnesis, then prescribe tests and examinations. An initial survey helps specialists predict the stage of development of the disease and its form. But for a more detailed picture, the following is carried out:
- Objective neurological examination. This inspection is carried out with a special hammer. The doctor evaluates the movement, tone and strength of the patient’s muscles, sensitivity (superficial and deep), nerve function, etc.;
- Laboratory diagnostics: general blood test (allows us to exclude a number of diseases similar in symptoms to MS);
- Lumbar puncture - taking fluid from the spinal cord. This analysis is mandatory if MS is suspected. Although this manipulation is unpleasant, it does not cause any harm to the spinal cord, and the discomfort disappears within a few days.
- Hardware diagnostics.
At the moment, specialists use the following hardware diagnostic methods:
- Superposition electromagnetic scanning is a modern method that allows one to determine the activity of enzymes in nervous tissue.
- Proton magnetic resonance spectroscopy - this procedure is used to assess the level of brain metabolism, as well as the state of the psyche.
- Magnetic resonance imaging is one of the most effective diagnostic methods: MRI images show the current state of the brain and problem areas, if any. Since the picture is taken in three projections, it is possible to see even the smallest plaques.
- Electroencephalography is a method that allows you to determine the state of brain activity and the integrity of nerve fibers. Since MS is often localized in the visual area, if symptoms are present, special attention is paid to it on the EEG.
- Differential diagnosis allows you to determine an accurate diagnosis by excluding diseases with a similar course.
Make an appointment
MRI for diagnosing MS
MRI is one of the most highly informative methods for diagnosing MS. It allows you to detect plaques on the surface of the brain, expansion of the cavity of the cerebral ventricles and atrophy of the cortex.
To make the image even more informative, contrast fluid is often used during MRI. It accumulates in places where myelin has been destroyed, and in the pictures such areas are visible even better.
Spinal puncture
This study is mandatory if MS is suspected, but requires psychological preparation of patients, since many fear possible damage to the spinal cord during manipulation. If the patient is sick, an increased number of lymphocytes and an increased level of immunoglobulins G will be detected in the cerebrospinal fluid (CSF). This test will help both in detecting MS and in excluding other diagnoses.
Study of bioelectrical activity of the brain
An electroencephalograph is a device that allows you to study signals from the central nervous structures of the brain. During the study, it is easy to determine the presence or absence of damage to nerve fibers, as well as their degree. Also, using this diagnostic method, you can monitor the effectiveness of treatment.
Complications, prognosis
If treatment is not started in a timely manner, or treatment does not take into account the type of multiple sclerosis, the risk of complications is high:
- bursts of causeless, uncontrollable laughter and crying,
- urological infections,
- bedsores,
- tremor,
- epileptic seizures;
- paralysis in the upper and lower limbs,
- trigeminal neuralgia,
- depression,
- diplopia - double vision,
- Lhermitte's symptom is paresthesia (a sudden feeling of intense burning) with a sensation of electric current passing through the back.
Despite the fact that the disease is not simple, for some patients we can confidently voice a favorable prognosis.
If previously, when a diagnosis of “multiple sclerosis” was made, disability began to develop in most patients within 3-5 years, but now, with properly selected medications, it is possible to delay the progression of the disease by 10 and sometimes 20 years.
But much depends on the form of sclerosis. One of the most insidious is the primary progressive form. At first, the symptoms are most vague. The diagnosis is often not made immediately, and treatment, accordingly, is also delayed. But there are often cases when, 10 years after the onset of the disease, the patient simply cannot take care of himself and finds it difficult to move.
At the same time, up to 50% of patients are faced with a form of natural progression. while maintaining the ability to work and practically the usual way of life. The only thing is that they cannot visit baths or stay in the heat for a long time. The main difficulty is to learn to accept your diagnosis and live with it.
Treatment
At the moment, treatment for MS is quite effective (10–20 years ago this disease led to disability in most cases), it includes:
- Drugs that change the course of multiple sclerosis and have a positive effect on the immune system.
- Hormonal agents. Designed to suppress exacerbations. It is worth noting that new hormones do not produce the same side effects as the previous generation of drugs.
- Exercise therapy is an important method in the treatment of MS, since the less the patient moves, the more muscle dystrophy develops.
- Drugs that restore nervous tissue are being developed (they are not currently registered in the Russian Federation)
The psychological attitude of the patient, the person’s readiness to overcome his illness every time it manifests itself again, is also very important.
The cost of treatment for multiple sclerosis in Moscow is calculated individually, as it may include different treatment regimens. An appointment with a neurologist starts from 5,150 rubles.
What is it[edit]
It’s like polyneuropathy, but not as usual in the legs/arms, but affecting the white matter in the head; Everything happens roughly reminiscent of the development of GBS: neurons lose their myelin sheath and nerve impulses begin to be lost, ping increases, the number of lost packets also increases - parts of the nervous system lose communication with each other.
Again, like GBS, this is lupus! autoimmune lesion (the most common one affecting the nervous system) [1]. That’s it, we don’t know anything else, what triggers it, or what provoking factors matter; so, little by little:
- for those living in industrial zones it occurs more often (yup, ecology!);
- viral/bacterial infections (hello, herpes) increase the likelihood;
- as well as injuries, stress, food and everything else.
People get it more often in the northern regions (vitamin D deficiency), although solar radiation is also a risk factor, but this does not equalize the statistics in the south.
It is not even clear whether the autoimmune reactions are primary or secondary, although they are unconditional and clearly expressed in the acute phase of the lesion, but whether the disease begins with them, or whether the whole point is in an unknown previous damage to the myelin is unclear, there is no one to blame yet. There is a certain twist about genetics, since the disease does not seem to be considered hereditary, but familial cases make up up to 10% percent, and some nations are more susceptible to it than others. [2]
In general, the coolest and most succinct description of the development of MS is expressed in one phrase: “the occurrence of this disease is associated with a random individual combination of unfavorable endogenous and exogenous risk factors”
. Wow, wow. You can't hide, everyone has a chance. All this and something else unknown leads to the formation of an inflammatory plaque, where myelin destruction, demyelination, occurs.
Occurs between 20 and 50 years, twice as often in women. [3]
McDonald[edit]
The most recent criteria for making a diagnosis named after MacDonald from 2010; the first two do not need additional data:
- two or more exacerbations + two or more lesions on imaging;
- two or more exacerbations + one or more lesions, but there is strong evidence of anamnestic data.
If there is only one exacerbation, or progression of symptoms without exacerbations, or if there is only one focus, one should look for distribution in time/space using MRA or waiting for the appearance of new exacerbations/foci.
MRI is the main method of objectively confirming the diagnosis, allowing you to see “black holes” in the head on T1 mode, or, conversely, bright spots on T2. Gadolinium contrast allows you to see even small lesions, but in general the main purpose of contrast is to determine the activity of the process and separate plaques into old and new.
Lumbar puncture most often becomes the icing on the cake of a completed diagnosis.
EDSS[edit]
Expanded Disability Status Scale - a rating by which patients are measured against each other on the topic of who is more or more ill. The interesting thing is that movement on the scale is not always inexorable-only forward; often people roll back to the recovery point with a lower score. The rating is of interest not only to doctors and their clients, but also to ordinary people, since it allows them to feel the frailty of life.
The assessment is made based on the number of affected functional systems and clinical manifestations:
- Sensitivity;
- Pyramid - walking;
- Cerebellum - coordination;
- Urinary and bowel control;
- Visual - vision;
- Brainstem - speech and swallowing;
- Mental;
- Other - any other neurological problems of MS, for example, fatigue.
The last two points are almost not taken into account, for which the scale is criticized - the same depression, like a violation of mental function, happens quite often and quite reduces activity, but is ignored by the point system.
0.0: Start: everything is fine. 1.0: Not disabled, but you can find a neurological deficit in one function (reduced vibration sensitivity, for example). 1.5: Still not disabled, but deficit affects more than one function. 2.0: Slightly disabled in one of the functions (constantly staggers a little when walking). 2.5: Slightly disabled in one function or slightly disabled in two. 3.0: Almost disabled by one, or slightly disabled by 3-4 (still ambulatory). 3.5: Almost one at a time + a little at 1-2; or almost two; or a little bit of five. 4.0: Already disabled, but ambulatory and satisfactory: he walks almost all day on his own, can pick up and walk half a kilometer without assistance/rest. 4.5: Same, can work with some restrictions/assistance and walk 300 meters without rest. 5.0: Forced march reduced to 200 meters, performance reserves require part-time work. 5.5: Hundred meters like Usain, only not fast and on foot, but without help. Full-fledged household activity is not excluded. 6.0: 100 meters with a stick only. 6.5: Cane/crutches/walker needed to cover 20 meters. 7.0: Movement damage radius is limited to five meters; When you have a “wheelchair” device, movement and activity are limited only by the lack of ramps. 7.5: A few steps at most, then only wheels with a motor as an assistant. 8.0: More immobile than movable and spends most of the time in bed/chair, but can care for himself. 8.5: Same, self-service is difficult. 9.0: Only bed, but can send you away to chat and eat. 9.5: Complete disability without communication and food, because he cannot swallow. 10.0: Finish and sad credits (no one knows the practical value of this point).
Treatment goals
Any woman with this diagnosis needs therapy. Her tasks:
- avoid exacerbations;
- eliminate exacerbation;
- improve the course of the disease;
- alleviate symptoms.
Treatment of exacerbation
Medicines from the glucocorticoid group (GCS) are used. They suppress immune responses. Their action in relation to MS:
- relieve inflammatory and autoimmune reactions;
- reduce the duration of exacerbation, but do not affect subsequent relapses;
- are not used long-term due to serious side effects.
If the course is malignant, in addition to GCS, cytostatics are prescribed.
Make an appointment
Multiple Sclerosis Modifying Drugs (MSMDs)
Modern and most effective treatments for MS. Their main effect is to improve the course of the disease. After taking DMTRS, the frequency of exacerbations decreases, the disease becomes more stable.
At the moment there are two PITRS lines:
- β-interferon preparations;
- Immunoglobulins, strong immunosuppressants, autologous bone marrow cell transplantation.
Symptomatic treatment
Patients with MS, in addition to specific treatment, require medications to relieve symptoms:
- Spasticity: muscle relaxants, M-anticholinergics, botulinum therapy.
- Epileptic seizures: anticonvulsants.
- Sleep problems: anxiolytics, sleeping pills.
- Bladder problems: anticholinesterase drugs.
- Depression, mood swings: antidepressants, mood stabilizers.
Any medicine is prescribed only by a doctor. Drugs from the above groups may be incompatible with each other! When prescribing, the doctor takes into account the patient’s condition, MRI results, laboratory values and side effects of various drugs.
Transcranial magnetic stimulation
A relatively new technique based on stimulating cells with a magnetic field. Used for both treatment and diagnosis.
- relieves muscle spasticity;
- determines the excitability of the cerebral cortex;
- acts precisely on individual zones of the cortex.
Disorders in the functioning of the pelvic organs
Sixty-eight percent of people with MS experience one or more types of pelvic floor abnormalities. Symptoms include loss or absence of bladder or bowel control: urinary incontinence, urinary frequency and urgency, bowel incontinence, sexual dysfunction, pelvic organ prolapse, and pelvic pain associated with a “spastic” pelvic floor.
The most common diagnosis among MS patients is a spastic (overactive) bladder. The organ is unable to hold a normal amount of urine in the bladder, which does not empty properly.
A spastic bladder is characterized by:
- private urination;
- hesitancy to start urinating;
- frequent night urination;
- urinary incontinence;
- inability to completely empty the bladder.
Healthy bladder function is important for long-term kidney health, infection prevention, personal independence, self-confidence and improved quality of life. Untreated bladder problems can cause:
- increasing weakness;
- Bladder and urinary tract infections (UTIs) or kidney stones, which cause serious pain and compromise your overall health;
- problems with work, home and social activities;
- loss of independence, self-esteem and self-confidence.
Early medical evaluation is important to determine the cause of bladder dysfunction and select appropriate treatments. More serious urinary problems can lead to blood and skin infections.
Complications of multiple sclerosis
MS itself has severe symptoms, the progression of which leads to disability. The most serious consequences of MS:
- Paralysis. The woman finds herself in a wheelchair and requires constant care.
- Pneumonia. It is often the cause of death in MS patients.
- Muscle weakness in walking patients increases the risk of falls and fractures, and in bedridden patients - the development of bedsores;
- With MS, irreversible changes occur in the brain, so the patient may become depressed: this complication occurs in approximately 50% of cases;
- Urinary system infections. They threaten with such a serious condition as urosepsis - the spread of infection from the urinary system throughout the body. Urosepsis is lethal.
- Urinary incontinence. An unpleasant symptom that makes life difficult.
- Complications from hormonal drugs. Long-term use of corticosteroids causes:
- osteoporosis - decreased bone density;
- stomach ulcer;
- decreased immunity;
- cataract.
- flu-like syndrome, manifested by chills and headache;
- changes in laboratory parameters (liver transaminases, platelets).
Cerebellar disorders
Coordination problems are common in multiple sclerosis and arise mainly from pathology in the cerebellum itself or when brain connections are disrupted. Patients may have either acute dysfunction associated with an acute exacerbation or chronic cerebellar problems with progressive disease.
Involvement of the cerebellar and brainstem connections occurs quite often during an exacerbation. Relapse of the cerebellum early in the development of the disease is associated with an increased risk of cerebellar damage during the subsequent course of MS. Experience shows that cerebellar involvement early in the disease worsens the prognosis. In a recent database study of approximately 15,000 patients who experienced a total of 50,000 exacerbations, cerebellar relapses accounted for approximately 10% of the total. They were more common in younger men and those with longer duration of progression.
It is estimated that 80% of patients with established MS experience tremors, which are especially common in patients with advanced disease. This is a consequence of unstable functioning of the cerebellum. Tremor can affect the limbs, trunk, vocal cords and head, but such a severe form is a relatively rare consequence of sclerosis.
Thus, cerebellar dysfunction may be a clear indicator of progressive MS. In general, this entails increased disability and poor prognosis.
Caring for sick women
Patients with MS need constant care, so if the patient has no relatives, he is often transferred to inpatient treatment. A patient with MS needs the following help:
- ensuring physical mobility to prevent muscle atrophy;
- walking assistance;
- control of the frequency of trips to the toilet;
- creating a positive emotional mood;
- light massage of the limbs (as recommended by a doctor), etc.
Make an appointment
What do the patient's relatives need to know?
It is worth remembering that MS is a disease that currently cannot be completely cured. But, at the same time, you should not treat a patient with multiple sclerosis as a disabled person. For a long time, people with this diagnosis are able to take care of themselves and even work, so do not interfere with this. Create an atmosphere of care and love around you: exercise with the patient, prepare food for him that corresponds to the diet prescribed by the doctor, and simply be there to help in moments of exacerbation of the disease.
Currently, patients with MS can live a full life up to 72-75 years, but only if treated and followed the doctor’s recommendations. How you can support the patient:
- Never say that recovery is possible; there is no need for false promises. Only stabilization and reduction of symptoms is possible.
- Encourage interest in treatment and rehabilitation. The Yusupov Hospital has a rehabilitation center for patients with MS. With the help of modern equipment and the use of new techniques, patients begin to feel more confident.
- Offer feasible tasks. This way the patient will feel needed and important.
- Do not scold the patient for clumsiness or inattention. These are symptoms of the disease. Man cannot control them in any way.
- Encourage the person to be physically active if possible.
- Control your diet. You should not eat food high in animal proteins and fats. Find the person an adequate replacement for his favorite products.
- Help me find friends. A person needs communication not only in his usual circle. If the patient cannot leave the house, you can find friends on social networks, for example, in multiple sclerosis groups. This way she will feel that she is not alone in her illness.
Several reasons why you will use our services
- Individual treatment and approach to each patient.
- Properly designed nutrition that benefits the patient.
- Professional service and care for a sick person.
- Convenient location of the guesthouse from the city.
- Safe accommodation in a boarding house is provided by a specialized security holding company.
- All treatment is carried out according to the developed programs of our specialists, who have received high awards from statesmen and received certificates from the country’s Ministry of Health.
- Our boarding house has a reputation for being honest and decent in serving its residents.
Multiple Sclerosis Center
Yusupov Hospital will be the best choice for the treatment of multiple sclerosis. Highly qualified neurologists with many years of experience work here. Patients receive not only medicinal and non-medicinal support (physiotherapy, massage, exercise therapy, etc.), but also psychological help, which is especially important for patients with multiple sclerosis. The hospital is equipped with the latest technology, specialists use the latest examination methods. The correct diagnosis will be made quickly, which means the patient will receive treatment sooner. It is in this case that the prognosis for MS is good: the person will be able to live normally, and the risk of disability will be minimized.
Conclusions:
- Multiple sclerosis is a pathology affecting the nervous system. It is based on damage to the sheaths of nerve fibers and disruption of impulse conduction.
- The disease is not hereditary, but with certain combinations of genes the risk is higher.
- Increased background radiation, intoxication, stress, and previous injuries can provoke the development of the disease.
- When the first symptoms of multiple sclerosis appear, it is important to consult a doctor promptly. It’s better to have it confirmed that it’s just overexertion and fatigue, and not to find yourself in a situation where one on one is the acute phase of the disease.
- With multiple sclerosis, the quality of life deteriorates significantly. First of all, because physical activity decreases. But, if previously multiple sclerosis was immediately a death sentence, now there are methods and drugs through which it is possible not only to relieve the symptoms of the disease, but also to slow down the development of the disease. Doctors have learned to keep the disease under control. With timely diagnosis and treatment, the pathology no longer negatively affects life expectancy.
- CT and laboratory diagnostics play an important role in diagnosis. When clarifying the diagnosis, it is essential where the problem areas are located: in the brain or spinal cord.
In the 5th hospital of the city, treatment of multiple sclerosis is one of the main profiles. The hospital base has expert-class equipment for diagnosing this disease. Consultations with experienced neurologists are available. Treatment is approached in a comprehensive manner. Drug therapy, massage, physical therapy, including cycling on special simulators, and hypobaric oxygenation sessions are organized.
Forecast
It is not yet possible to completely eliminate the symptoms of MS, but maintenance therapy will help prevent the onset of disability, which in itself is very important. It is necessary to remember the following risks for patients diagnosed with MS:
- before 15 and after 40 years, the risk of complications increases;
- mental disorders or concomitant disorders/diseases can hasten death;
- disruptions in the functioning of vital organs (kidneys, lungs, heart) can lead to instant death.
To prevent any of this from happening, you need to constantly monitor the patient’s condition and consult a specialist in time to prevent complications. As for the life expectancy of people with MS, much depends on how quickly the correct diagnosis was made. A diagnosis made at an early stage and proper treatment are the key to a long and happy life for the patient.
Doctor, what will happen to me?[edit]
Thanks to advances in alternative medicine science, MS reduces life expectancy by only 5-10 years compared to the rest of the population. However, life will not be sugar, but for whom is it sweet? The disease occurs in both the poor and the rich (NHL hockey player Josh Harding was diagnosed with the condition in 2012, a year later he received a prestigious award and still continues to play), and in the children of celebrities, for example, the son of Ozzy Osbourne. About a third of people with SD live relatively normal lives without significant accumulation of deficits (and without disability) over the course of their lives.
Comparing any other chronicle with the topic of the article, the latter has a fairly large community of users of active people who search for information together and support each other, which is not at all surprising - the debut occurs at the most active age. They almost look like they are pregnant, especially considering that there are more women among the patients, who from time to time are actually pregnant.
Treatment[edit]
The therapy is specific, narrowly targeted and limited to drugs that can be counted on one hand, and then with the same fingers one can point to the sky which option will work. This is the gold standard, a classic (having hundreds of studies and approved by the FDA/EMA) and the only hope, also called “DITs” - drugs that modify the course of MS.
- Interferons:
- beta-1a - Avonex, Rebif, Genfaxon, Synnovex (the latter is recommended by patients to inject terrorists sentenced to death, because it is a low-quality generic; although some are satisfied, the taste and color of all interferons are different);
- beta-1b - Betaferon, Extavia, Ronbetal, Infibeta. First generation, the oldest drugs with a bunch of side effects.
- Chemotherapy (antitumor - it treats lymphomas, leukemia, prostate cancer, breast cancer):
- Mitoxantrone (Novantron, Oncotron). Due to significant side effects, it is used primarily for SPMS, PRMS, and rapid progression of RRMS.
- The most pathogenetic drug that blocks autoimmune reactions:
- Glatyromeracetate (Copaxone) is perhaps the only drug in general that can seriously be called immunomodulatory. It often causes allergic reactions, which is contraindicated for the target group, although the effectiveness of the drug is excellent.
- Antibodies are the last word in treatment, which gives some optimism:
- Natalizumab (Tysabri);
- Fingolimod (Gilenya);
- Daclizumab (Zenapax);
- Ofatumumab (Arzerra);
- Alemtuzumab (Campas);
- Ocrelizumab (Ocrevus)
- Rituximab.
- Steroids:
- in the form of pulse therapy during exacerbation: for example, methylprednisolone (Solu-Medrol);
- or in the form of ACTH analogues (Tetracosactide/Synacthen), which stimulate the synthesis of GCS in the adrenal glands.
All of them are used only by injection, cost a lot of money (compare with interferons and immunomodulators for acute respiratory viral infections - do you think people on DMT suffer from colds less?) and some have unpleasant effects, incl. interferons cause a flu-like condition, which necessitates a whole ritual of drug administration - the “dry needle rule”: after drawing the drug into the syringe, it is necessary to change the needle to a clean one; increase the dosage gradually over weeks; half an hour before the injection, take paracetamol/ibuprofen.
There are also a couple of unclassified drugs that are approved and well used: Teriflunomide (Abagio) - an inhibitor of the mitochondrial enzyme DHO-DG and Dimethyl fumarate (Tecfidera) - somehow an immune system suppressor.
When traveling, people have to carry medicines with them in thermal bags because they need cool storage.
Dietary supplement[edit]
Main article
:
Dietary supplement
Thanks to the unpredictable cyclical nature of the disease (in the case of the most common RRMS), people can be treated for a long time with untested remedies and say, “Here, it’s been 2 years without exacerbations!” I just want to be happy for them, but this never means that the methods used somehow contribute to this.
One can understand patients that they are not very happy with the current state of pharmacology, but it is what it is; Unfortunately, given the small number of drugs, people often find themselves in the tenacious hands of dietary supplement makers who offer a lot of neuroprotectors, antioxidants and other useless pills that only play on trust and hopes. It is worth understanding that this is not at all a disease where you can experiment with treatment, especially with untested drugs.
| I have been in an international company for 3 years, which has been on the market for 15 years. And I take our products - these are dietary supplements. With their help, I improved a lot in my body. But recently I was diagnosed with optic nerve MS, I purchased all the products that are necessary for MS. I only take them and have decided to refuse drug treatment, which the doctor is supposed to prescribe for me tomorrow. I believe that I can cope with this illness. Don’t be afraid of dietary supplements, dietary supplements are great. You just need to find quality ones and know how and when to take them. |
| a typical patient who has found faith in dummies (that’s exactly what you shouldn’t do). |
There are no “proven dietary supplements”: a substance has either been tested, works and is a medicine, or its manufacturer is somewhat obscure, not wanting to register it as a normal drug.
Prevention
Since at the moment science has difficulty determining the exact causes of MS, there are no specific preventive measures. But one thing is for sure - maintaining a healthy lifestyle is an excellent preventive measure for most diseases. Namely:
- play sports (it’s enough to run in the morning or do exercises);
- avoid stress;
- give up bad habits;
- normalize nutrition and weight;
- sleep at least 8 hours a day;
- Be periodically examined by a neurologist.
Such simple rules are suitable for both healthy people and those already suffering from multiple sclerosis: it is important for them not to aggravate the course of the disease.
Professional care at the Vesna boarding house
Caring for a patient with multiple sclerosis is a difficult task. We understand the relatives of such a patient, therefore, we offer high-quality services for this event. Since the patient is in a helpless state, our staff will do everything to make him feel comfortable and undergo all the treatment measures prescribed by our doctors.
Why is it difficult to care for a person diagnosed with multiple sclerosis? The whole point is that:
- the patient constantly experiences chronic fatigue;
- constantly forgets everything he knows or has learned in a day;
- confuses the sequence of his actions;
- violates the use of medication doses and the time of taking them.
A patient in such a situation requires constant help and moral support. Our employees will give everything your relative needs and brighten up his loneliness.
Providing patronage services
When providing care services, there are standard types of responsibilities:
- when moving, the patient is provided with the necessary special medical equipment;
- exercising full control over the use of medications;
- constant change of linen;
- Clothing repair;
- daily walks;
- accompanying the ward to physical procedures;
- assistance with eating;
- haircut and other hygiene services.
In addition, there are additional services, but this is discussed with the boarding house management.
Doctors' recommendations
Recommendations for women with multiple sclerosis:
- Avoid infections. They adversely affect the course and occurrence of exacerbations.
- Lead an active lifestyle, but make sure there is no excessive physical activity or overwork. Any physical activity should be discussed with your doctor in advance.
- Do not visit the sauna and bathhouse, do not take hot baths. High temperatures provoke exacerbations.
- Give up bad habits - they contribute to exacerbations.
- Follow the principles of nutrition for MS. It is necessary to avoid animal fats and proteins, reduce the amount of fat in food, and include foods high in vitamin D in the diet.
- Follow the recommendations of your doctor. Don't forget to take your medications.
- Attend a rehabilitation center. Talk to a psychologist about your state of mind.
If you suspect multiple sclerosis or for the treatment and rehabilitation of patients with this diagnosis, you can contact the Yusupov Hospital in Moscow.
Make an appointment
Sensory impairment
A unique aspect of the symptoms of multiple sclerosis is the extremely common temperature sensitivity of patients whose neurological symptoms are temporarily aggravated by an increase (or decrease) in body temperature.
Heat sensitivity, or Uthoff's phenomenon, occurs in 60–80% of patients with this disease. An increase in body temperature may cause temporary deterioration, usually associated with exposure to a warm environment or exercise, and lasts until core temperature returns to baseline. However, a decrease in body temperature as a result of taking cold baths or exposure to low ambient temperatures can also provoke a worsening of the clinical picture of the pathology.
Episodes of temperature sensitivity among patients with sclerosis are also known as pseudoexacerbations or pseudorelapses. Although the increase in symptoms may be similar in nature to those that occur during an exacerbation, the worsening of the condition is not associated with the active progression of the disease and is temporary. Moreover, the symptoms return to normal when the internal temperature is restored. Therefore, the patient experiences significant difficulties in maintaining an appropriate level of physical activity
Symptoms
Symptoms of multiple sclerosis most often appear between the ages of 20 and 40. Typically, a person notices symptoms after developing two or more different episodes of symptoms before MS is suspected.
The most common early symptoms of MS include:
- Tingling
- Numbness
- Body imbalance
- Weakness in one or more limbs
- Decreased vision or diplopia
- Other symptoms that are much less common are:
- Slurred speech
- Sudden onset of paralysis
- Impaired coordination of movements
- Cognitive impairment
As the disease progresses, symptoms such as spasticity, sensitivity to heat, fatigue, changes in thinking or perception, and sexual dysfunction appear.
- Fatigue. This is a characteristic and common symptom of MS. It usually appears in the afternoon and can be manifested by severe muscle weakness, mental fatigue, drowsiness. Feelings of physical exhaustion are not related to the amount of work done and many MS patients complain of extreme fatigue, even after getting enough sleep.
- Sensitivity to high temperature. Heat sensitivity: The onset or worsening of symptoms after exposure to heat (such as after showering) occurs in most people with MS.
- Muscle spasticity. Muscle spasticity is a common and often debilitating symptom of MS. Muscle spasticity usually affects the muscles of the legs and arms, and can affect the motor ability of the limbs.
- Dizziness. Many patients with multiple sclerosis experience a feeling of dizziness. The occurrence of this symptom is associated with a disturbance in the transmission of nerve impulses in a complex system that ensures body balance (vision, proprioception, etc.)
- Cognitive impairment. Problems with thought processes occur in about half of people with MS. There is a disturbance in concentration and memory impairment. 10% of patients experience severe cognitive impairment and lose the ability to care for themselves.
- Visual impairment. Vision problems are quite common in patients with MS. Visual impairment is mainly associated with optic neuritis and occurs in 55% of cases. As a rule, visual impairment rarely leads to complete blindness.
- Pathological sensations. Many patients experience various pathological sensations such as tingling with pins, itching, and pinpoint pain. As a rule, these symptoms are not life-threatening and can be relieved quite well with treatment.
- Speech and swallowing disorders. Some patients have problems with both swallowing and speech. This is due to damage to the nerves responsible for these functions.
- Tremor. This symptom is quite common in patients with multiple sclerosis and, unfortunately, is difficult to treat.
- Walking disorder. Gait disturbance is a fairly common symptom in multiple sclerosis. This is mainly due to muscle weakness or muscle spasticity. In addition, the cause may be a lack of coordination and balance of the body.
Rare symptoms of multiple sclerosis include breathing problems and seizures.
Symptoms fall into three categories: primary, secondary, and tertiary.
The main symptoms are a direct result of the demyelination process. Demyelination impairs the transmission of electrical signals to muscles (allowing muscles to perform motor function) and body organs (allowing them to perform their normal functions.) Symptoms include: weakness, tremors, tingling, numbness, balance problems, blurred vision, paralysis, and problems with function bladder or intestines. Modern treatments can control these symptoms.
Secondary symptoms are a consequence of the primary symptoms. For example, paralysis (the main symptom) can lead to bedsores, and bladder dysfunction can cause frequent, recurring urinary tract infections. These symptoms can also be treated, but the main goal is to prevent complications from occurring.
Tertiary symptoms are social, psychological, and professional-labor symptoms arising as a result of the patient’s disability and loss of ability to work to one degree or another. Depression, for example, is quite common in patients with multiple sclerosis.
Unfortunately, each patient’s symptoms manifest themselves differently, as does the progression of the disease. Some patients may have mild symptoms for years without progression. In other cases, the disease can progress rapidly over several months. And with a variety of symptoms, some may have some symptoms and not others.