SPECIALISTS Gynecologist Gynecologist-endocrinologist Pediatric gynecologist Mammologist-oncologist Dermatologist Hirudotherapist Intimate plastic surgery Doctor Contour plastic doctor Ultrasound doctor SERVICES AND PRICES Gynecology Mammology Ultrasound diagnostics Paid tests Intimate surgery Contour plastic Treatment for women PROMOTIONS AND DISCOUNTS Students Teams Friends and subscribers am For residents of the region For pensioners Promotions in clinic
Gynecologists consider taking properly selected hormonal contraceptives to be one of the most effective ways to avoid unplanned pregnancy. The incredible number of them in pharmacies does not allow modern women to focus on a specific choice, and can lead to erroneous preferences. Often, ignorance of the types of contraceptives is fraught with unpleasant consequences. Many people don’t know anything else except condoms and intrauterine devices. Today we will talk about oral contraceptives and how to make the right choice.
The birth control pill is a drug that you take once a day. There are several types of them. Combined oral contraceptives contain estrogens and gestagens, which suppress ovulation. The so-called “mini-pills” contain only 1 hormone, gestagen, and are an alternative if estrogens are contraindicated.
Highest efficiency 99% In cases of 100% correct use, in strict accordance with the instructions, approximately only 1 in 100 women will experience an unplanned pregnancy per year. For comparison, without contraception, 85 out of 100 women will experience an unplanned pregnancy over the same time period.
Combined oral contraceptives (COCs)
Most drugs use the estrogen ethinyl estradiol at a dosage of 20 mcg. The following is used as a gestagen:
- norethindrone;
- levonorgestrel;
- norgestrel;
- norethindrone acetate;
- norgestimate;
- desogestrel;
- Drospirenone is the most modern progestin.
A new trend in the production of COCs is the release of drugs that increase the level of folate in the blood.
These COCs contain drospirenone, ethinyl estradiol and calcium levomefolate (a metabolite of folic acid) and are indicated for women planning a pregnancy in the near future. Monophasic COC contraceptives have a constant dose of estrogen and progestin. Biphasic COCs contain two, triphasic - three, and four-phase - four combinations of estrogen and progestogen. Multiphasic drugs have no advantages over monophasic combined oral contraceptives in terms of effectiveness and side effects [1].
About three dozen COCs are available on the pharmaceutical market, the vast majority of which are monophasic. They are available in the form of 21+7:21 hormonally active tablets and 7 placebo tablets. This facilitates consistent daily monitoring of regular COC use.
Combined oral contraceptives (COCs) list: types and names
Mechanism of action
The main principle of operation of COCs is to inhibit ovulation. The drugs reduce the synthesis of FSH and LH. The combination of estrogen and progestin gives a synergistic effect and increases their antigonadotropic and antiovulatory properties. In addition, COC contraceptives change the consistency of cervical mucus, cause endometrial hypoplasia and reduce contractility of the fallopian tubes.
Efficiency largely depends on compliance. The pregnancy rate during the year ranges from 0.1% with correct use to 5% with violations of the dosage regimen.
Advantages
Combined hormonal contraceptives are widely used to treat menstrual irregularities and reduce or eliminate ovulatory syndrome. Taking COCs reduces blood loss, so it is advisable to prescribe them for menorrhagia. COCs can be used to adjust the menstrual cycle - if necessary, delay the onset of the next menstruation.
COCs reduce the risk of developing benign breast formations, inflammatory diseases of the pelvic organs, and functional cysts. Taking COCs for existing functional cysts helps to significantly reduce them or completely resolve them. The use of COCs helps reduce the risk of malignant ovarian diseases by 40%, endometrial adenocarcinoma - by 50% [2]. The protective effect lasts up to 15 years after discontinuation of the drug.
Flaws
Side effects: nausea, breast tenderness, breakthrough bleeding, amenorrhea, headache.
Estrogen, which is part of COCs, can activate the blood clotting mechanism, which can lead to the development of thromboembolism. The risk group for developing such complications while taking COCs includes women with high levels of LDL and low levels of HDL in the blood, severe diabetes accompanied by arterial damage, uncontrolled arterial hypertension, and obesity. In addition, the likelihood of developing blood clotting disorders increases in women who smoke.
Contraindications for the use of combined oral contraceptives
- thrombosis, thromboembolism;
- angina pectoris, transient ischemic attacks;
- migraine;
- diabetes mellitus with vascular complications;
- pancreatitis with severe triglyceridemia;
- liver diseases;
- hormone-dependent malignant diseases;
- bleeding from the vagina of unknown etiology;
- lactation.
COCs and breast cancer
The most comprehensive analysis of cases of breast cancer development while taking COCs was presented in 1996 by the Collaborative Group on Hormonal Factors in Breast Cancer [3]. The study assessed epidemiological data from more than 20 countries. The study results showed that women who are currently taking COCs, as well as those who have taken them in the past 1–4 years, have a slightly increased risk of developing breast cancer. The study highlighted that women participating in the experiment were much more likely to undergo breast examinations than women not taking COCs.
Today it is assumed that the use of COCs may act as a cofactor that only interacts with the underlying cause of breast cancer and possibly potentiates it [2].
How to choose birth control pills
There are many different types of birth control pills, and each one is slightly different. The main thing is to strictly follow the instructions that come with them. It is important to take them correctly, since missing them or not taking them on time weakens the effectiveness of the protection. Selection of oral contraceptives in the clinic will allow a woman to correctly choose for herself exactly those hormonal pills that will potentially have minimal risks of developing adverse reactions to their use.
Adolescents are prescribed drugs with an antiandrogenic effect. They help get rid of skin rashes and significantly improve a girl’s mood. Before menstruation, taking such drugs reduces pain in the lower back and legs.
Properly selected contraceptive pills and COCs do not have a negative effect on fertility in the future (it is restored in most cases within the first 3 months after discontinuation of the drug). Accidental use of modern hormonal contraceptives in the early stages of pregnancy does not produce a mutagenic or teratogenic effect and does not require its interruption.
The drug can be considered suitable if, after an adaptation period of three months, the release of blood completely stops in the middle of the menstrual cycle. If you have any questions during their use, contact your gynecologist-endocrinologist for additional advice. It is unlikely that you will be able to select contraceptives on your own or using online tests, because all drugs have different compositions, just as a woman may have certain indications and contraindications.
How to choose the right hormonal pills according to your phenotype
Phenotype is the properties and characteristics of an organism as a whole, which have developed during the process of its growth and development. Each of them has certain characteristics that will help you choose birth control pills.
There are three phenotypes of the female body:
- Estrogenic;
- Progesterone.
- Balanced.
1. Estrogen type. The estrogenic phenotype of the female body is characterized by:
♦ woman’s height—average or short; ♦ voice – deep feminine; ♦ skin and hair are dry; ♦ breasts - well developed and enlarge before menstruation; ♦ the pubis is covered with female-type hair; ♦ menstruation - more than 5 days and heavy; ♦ PMS - nervousness and tension; ♦ menstrual cycle - more than 28 days; ♦ leucorrhoea - abundant; ♦ pregnancy - without pronounced complications.
2. Progesterone type. Girls with a progestin type of appearance have the following features:
♦ height - average or high; ♦ low timbre; appearance - masculine features; ♦ breast – underdeveloped; ♦ pubic hair - male type; ♦ skin and hair are oily and prone to rashes; ♦ menstruation - less than 5 days, scanty; ♦ PMS - depression, pain in the muscles of the legs, lower back and abdomen; ♦ menstrual cycle - less than 28 days; ♦ leucorrhoea - scanty; ♦ pregnancy - toxicosis and significant weight gain.
3. Balanced type . This female phenotype is characterized by:
♦ height - average; ♦ voice – feminine; ♦ skin and hair - normal; ♦ chest - moderately developed; ♦ pubic hair - female type; ♦ menstruation - 5 days and moderate; ♦ PMS - without obvious physical manifestations, mood swings; ♦ menstrual cycle - 28 days; ♦ leucorrhoea - moderate; ♦ the course of pregnancy is normal.
TABLETS BY PHENOTYPE
✅ Women of the estrogenic type can choose oral contraceptives “Mikrogynon”, “Sileste”, “Miniziston 20”, “Rigevidon”. ✅ The balanced type can use “Miniziston”, “Tri-mercy”, “Tri-zitron”, “Tri-regol” and others. ✅ Progesterone type is recommended to take “Balara”, “Janine”, “Klaira”, “Yarina” tablets.
Tests for selecting birth control pills
Do you want to start taking birth control pills? A good gynecologist at our clinic will tell you which ones are best to choose after undergoing tests and examination. The choice of contraceptives is individual for each woman and depends on the general condition of the body, data on previous diseases and the presence of existing gynecological problems. This will help the doctor exclude contraindications to taking oral contraceptives and determine your phenotype. Depending on these factors, gynecologists-endocrinologists choose birth control pills.
What tests need to be taken for hormonal pills:
✔ Gynecological examination on a chair; ✔ Extended colposcopy with Schiller test; ✔ Oncocytology of the cervix; ✔ Blood tests for hormonal levels (FSH, LH, prolactin, progesterone, estradiol, testosterone, DHEA sulfate, 17-OH-progesterone, etc.); ✔ Biochemical blood test (liver tests, cholesterol, triglycerides, sugar, etc.); ✔ Analysis of hemostasis (clotting - fibrinogen, PTI, thrombin time); ✔ Consultation with a mammologist ✔ Ultrasound of the mammary glands; ✔ Ultrasound of the pelvic organs.
Thus, given the fairly wide range of hormonal contraceptives on pharmacy counters and the presence of contraindications to their use, consultation with a doctor is required. We decided to take birth control pills - our specialist will tell you what tests to take! This will protect you from making the wrong choice of contraceptives and prevent unwanted consequences. Examination of women's health before prescribing contraceptives allows you to choose the most effective means to prevent unwanted pregnancy!
Therefore, if you are faced with the question of which contraceptives are better and how to choose a contraceptive without health consequences, do not self-diagnose and do not make a choice yourself! Contraceptives that are well tolerated by your friends do not guarantee that they will suit you and will not cause unwanted side effects. Entrust such a serious issue to the professionals. We invite you to make an appointment with a gynecologist-endocrinologist right now!
How much does it cost to choose hormonal pills?
| Service | Price |
| Consultation with a gynecologist-endocrinologist | 2 500 |
| Pelvic ultrasound | 3 000 |
| Colposcopy | 1 500 |
| Oncocytological screening of the cervix | 4 500 |
| Blood tests for hormones, 1 unit. | 490 |
| Blood test for biochemistry, 1 unit. | 250 |
| Hemostasis analysis (coagulogram) | 1 250 |
| Appointment with a mammologist-oncologist | 2 500 |
| Ultrasound of the mammary glands | 2 500 |
| Selection of contraceptive pills in the clinic based on the results of tests and examinations performed | 1 500 |
Tired of birth control pills? What could be better:
| Intrauterine devices | Subcutaneous implant |
There may be contraindications, consult a specialist before using oral contraceptives. The list of tests for selecting birth control pills may vary depending on your health condition. All prices indicated on the site are provided as reference information, are not a public offer and are subject to change without prior notice. For detailed information about the cost of services, please contact the reception staff.
Transdermal Therapeutic System (TTS)
The transdermal therapeutic system patch is applied for 7 days. The used patch is removed and immediately replaced with a new one on the same day of the week, on the 8th and 15th days of the menstrual cycle.
TTS appeared on the market in 2001 (“Evra”). Each patch contains a week's supply of norelgestromin and ethinyl estradiol. TTC is applied to dry, clean skin of the buttocks, abdomen, outer surface of the upper arm or torso with minimal hair growth. It is important to monitor the density of TTC attachment every day and not apply cosmetics nearby. Daily release of sex steroids (203 mcg norelgestromin + 33.9 mcg ethinyl estradiol) is comparable to that of low-dose COCs. On the 22nd day of the menstrual cycle, the TTS is removed and a new patch is applied 7 days later (on the 29th day).
The mechanism of action, effectiveness, disadvantages and advantages are the same as those of COCs.
Vaginal ring
The hormonal vaginal ring (NovaRing) contains etonogestrel and ethinyl estradiol (daily release 15 mcg + 120 mcg, respectively). The ring is installed for three weeks, after which it is removed and a week-long break is maintained. On day 29 of the cycle, a new ring is inserted.
The dosage of ethinyl estradiol in the vaginal ring is lower than that of COCs, due to the fact that absorption occurs directly through the vaginal mucosa, bypassing the gastrointestinal tract. Due to the complete suppression of ovulation and regular release, independent of the patient, the effectiveness is higher than that of COCs (0.3–6%). Another advantage of the ring is the low likelihood of dyspeptic side effects. Some patients experience vaginal irritation and discharge. In addition, the ring may accidentally slip out.
The effect of hormonal contraceptives on libido has not been sufficiently studied; research data are contradictory and depend on the average age in the sample and gynecological diseases, the drugs used, and methods for assessing the quality of sexual life. In general, 10–20 percent of women may experience a decrease in libido while taking medications. In most patients, the use of GCs does not affect libido [10].
Acne and hirsutism usually have low levels of sex hormone binding globulin (SHBG). COCs increase the concentration of this globulin, having a beneficial effect on the condition of the skin.
Hormonal contraceptives: how do they work?
OCs contain synthetic hormones - estrogen and progesterone. They inhibit ovulation - that is, they do not allow the egg to mature and exit into the fallopian tube. In addition, these same hormones prevent the sperm from meeting the egg and securing the fertilized egg in the uterus: the mucus becomes thick, the endometrium changes structure. This is the reason for such high efficiency - it reaches 98%. Thus, out of 100 women, pregnancy is possible in only two.
Some gynecologists are confident that taking OCs should be constant if a woman is not planning a pregnancy. But won't this cause harm to health?
Subtleties of application
Estrogen in COCs helps eliminate LDL and increase HDL and triglyceride levels. Progestins counteract estrogen-induced changes in lipid levels in the body.
- For acne, medications containing cyproterone acetate, drospirenone or desogestrel are prescribed as a progestin. COCs containing cyproterone acetate and ethinyl estradiol are more effective for acne than the combination of ethinyl estradiol and levonorgestrel [4].
- For hirsutism, medications containing progestogens with antiadrogenic properties are recommended: cyproterone acetate or drospirenone [5].
- Combinations of estradiol valerate and dienogest are more effective in reducing menstrual blood loss than ethinyl estradiol and levonorgestrel [6]. In addition, the intrauterine system is indicated for the treatment of menorrhagia.
- Preparations containing drospirenone 3 mg and ethinyl estradiol 20 mcg are recognized as the most effective combination for correcting PMS symptoms, including those of a psychogenic nature [7].
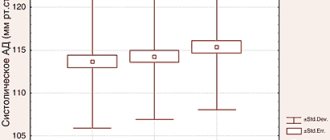
- Taking oral contraceptives increases systolic blood pressure (BP) by 8 mmHg. Art., and diastolic - by 6 mm Hg. Art. [8]. There is evidence of an increased risk of cardiovascular events in women taking COCs [9]. Due to the increased likelihood of developing myocardial infarction and stroke in patients with arterial hypertension, when prescribing COCs, the benefit/risk ratio must be carefully weighed.
- In non-smoking women under 35 years of age with compensated hypertension, COCs can be prescribed with careful monitoring of blood pressure during the first months of use.
- In cases of increased blood pressure while taking COCs or in women with severe hypertension, an intrauterine system or DMPA is indicated [10].
- The selection of a contraceptive for patients with dyslipidemia must be carried out taking into account the effect of the drugs on lipid levels (see Table 5).
- Because the absolute risk of cardiovascular events in women with controlled dyslipidemia is low, COCs containing 35 mcg or less of estrogen can be used in most cases. For patients with LDL levels above 4.14 mmol/l, alternative means of contraception are indicated [8].
- The use of COCs in women with diabetes mellitus accompanied by vascular complications is not recommended [2]. A suitable option for hormonal contraception for diabetes mellitus is the intrauterine levonorgestrel-releasing system, and, as a rule, no dose adjustment of hypoglycemic drugs is required.
- The results of epidemiological studies examining the risk of myocardial infarction when oral contraceptives are prescribed to women who smoke are contradictory. Due to limited convincing data, COCs are recommended to be prescribed with caution to all women over 35 years of age who smoke.
- Obesity with a body mass index of 30 kg/m2 and above reduces the effectiveness of COCs and transdermal GCs [8]. In addition, the use of COCs in obesity is a risk factor for venous thromboembolism. Therefore, the method of choice for such patients is mini-pills (gestagen-containing tablet contraceptives) and intrauterine contraceptives (levonorgesterel-releasing system).
- Use of COCs with estrogen dosages of less than 50 mcg in nonsmoking, healthy women over 35 years of age may have beneficial effects on bone density and vasomotor symptoms during perimenopause [8]. This benefit must be considered in light of the risk of venous thromboembolism and cardiovascular factors. Therefore, women of the late reproductive period are prescribed COCs individually.
List of sources
- Van Vliet HAAM et al. Biphasic versus triphasic oral contraceptives for contraception //The Cochrane Library. — 2006.
- Omnia M Samra-Latif. Contraception. Available from https://emedicine.medscape.com
- Collaborative Group on Hormonal Factors in Breast Cancer. Breast cancer and hormonal contraceptives: collaborative reanalysis of individual data on 53,297 women with breast cancer and 100,239 women without breast cancer from 54 epidemiological studies. Lancet 1996; 347(9017):1713–1727.
- Carlborg L. Cyproterone acetate versus levonorgestrel combined with ethinyl estradiol in the treatment of acne. Results of a multicenter study. Acta Obstetricia et Gynecologica Scandinavica 1986;65:29–32.
- Batukan C et al. Comparison of two oral contraceptives containing either drospirenone or cyproterone acetate in the treatment of hirsutism. Gynecol Endocrinol 2007;23:38–44.
- Fruzzetti F, Tremollieres F, Bitzer J. An overview of the development of combined oral contraceptives containing estradiol: focus on estradiol valerate/dienogest. Gynecol Endocrinol 2012;28:400–8.
- Lopez LM, Kaptein AA, Helmerhorst FM. Oral contraceptives containing drospirenone for premenstrual syndrome. Cochrane Database Syst Rev 2012.
- Armstrong C, Coughlin L. ACOG releases guidelines on hormonal contraceptives in women with coexisting medical conditions. — 2007.
- Carr BR, Ory H. Estrogen and progestin components of oral contraceptives: relationship to vascular disease. Contraception 1997; 55:267–272.
- Burrows LJ, Basha M, Goldstein AT. The effects of hormonal contraceptives on female sexuality: a review. The journal of sexual medicine 2012; 9:2213–23.