Instructions for use WARFARIN
It is not recommended to start or stop taking other medications, or change the dosage of medications taken, without consulting your doctor. When prescribing simultaneously, it is also necessary to take into account the effects of stopping the induction and/or inhibition of the action of Warfarin by other drugs.
The risk of severe bleeding increases when taking Warfarin simultaneously with drugs that affect platelet levels and primary hemostasis:
- acetylsalicylic acid, clopidogrel, ticlopidine, dipyridamole, most NSAIDs (except COX-2 inhibitors), penicillin antibiotics in high doses.
You should also avoid the combined use of Warfarin with drugs that have a pronounced inhibitory effect on the cytochrome P450 system, for example, cimetidine and chloramphenicol, when taken for several days the risk of bleeding increases. In such cases, cimetidine can be replaced, for example, with ranitidine or famotidine.
The effect of Warfarin may be enhanced when taken simultaneously with the following medications; Acetylsalicylic acid, allopurinol, amiodarone, azapropason, azithromycin, alpha and beta-interferon, amitriptyin, bezafibibrat, vitamin A, vitamin E, glibenclamide, glucagon, hemfibrosil, heparin, Grepafsacin, Danazole, derthoproopen, diazopoxin, digoxyide, digoxid , dizopiramid, disulfits, zafirlukast, indomethacin, ifosfamide, itraconazole, ketoconazole, clarithromycin, clofibrate, codeine, levamisole, lovastatin, methovasone, methotrexate, metronidazole, miconazole (including in the form of oral gel), nalidixic acid, norfloxacin, ofloxacin, omeprazole, oxyphenbutazone, paracetamol (especially after 1-2 weeks of continuous use), paroxetine, piroxicam, proguanil, propafenone, propranolol, influenza vaccine, roxithromycin, sertraline, simvastatin, sulfafurazole, sulfamethizole, sulfamethoxazole-trimethoprim, sulfafenazole, sulfinpyrazone, sulindac, steroid hormones ( anabolic and/or androgenic), tamoxifen, tegafur, testosterone, tetracyclines, thienylic acid, tolmetin, trastuzumab, troglitazone, phenytoin, phenylbutazone, fenofibrate, feprazone, fluconazole, fluoxetine, fluorouracil, fluvastatin, fluvoxamine, flutamide, quinine, quinidine, chloral hydrate , chloramphenicol, celecoxib, cefamandole, cephalexin, cefmenoxime, cefmetazole, cefoperazone, cefuroxime, cimetidine, ciprofloxacin, cyclophosphamide, erythromycin, etoposide, ethanol.
Preparations of some medicinal plants (official or unofficial) can also enhance the effect of Warfarin:
- for example, ginkgo (Ginkgo biloba), garlic (Allium sativum), angelica sinensis (Angelica sinensis), papaya (Carica papaya), sage (Salvia miltiorrhiza);
- and reduce: for example, ginseng (Panax ginseng), St. John's wort (Hypericum perforatum).
Warfarin and any St. John's wort preparations should not be taken at the same time, but it should be taken into account that the inducing effect of Warfarin may persist for another 2 weeks after stopping the use of St. John's wort preparations. If the patient is taking St. John's wort preparations, MHO should be measured and discontinuation. MHO monitoring must be careful because... its level may increase when St. John's wort is discontinued. After this, Warfarin can be prescribed.
Quinine contained in tonic drinks can also enhance the effect of Warfarin.
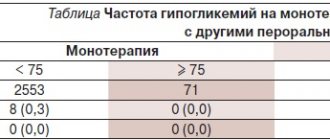
Warfarin may enhance the effect of oral sulfonylurea hypoglycemic agents.
The effect of Warfarin may be weakened when taken simultaneously with the following drugs:
- azathioprine, aminoglutethimide, barbiturates, valproic acid, vitamin C, vitamin K, glutethimide, griseofulvin, dicloxacillin, disopyramide, carbamazepine, cholestyramine, coenzyme Q10, mercaptopurine, mesalazine, mianserin, mitotane, nafcillin, primidone, retinoid, ritonavir, rifampicin, rofecoxib, spironolactone, sucralfate, trazodone, phenazone, chlordiazepoxide, chlorthalidone, cyclosporine. Taking diuretics in the case of a pronounced hypovolemic effect can lead to an increase in the concentration of clotting factors, which reduces the effect of anticoagulants. In the case of combined use of Warfarin with other drugs indicated in the list below, it is necessary to monitor MHO at the beginning and end of treatment, and, if possible, after 2-3 weeks from the start of therapy.
Foods rich in vitamin K weaken the effect of Warfarin; Decreased absorption of vitamin K caused by diarrhea or laxatives potentiates the effect of warfarin. Most vitamin K is found in green vegetables, so when treating with Warfarin, you should eat the following foods with caution:
- amaranth greens, avocado, broccoli, Brussels sprouts, cabbage, canola oil, chayo leaf, onion, coriander (cilantro), cucumber peel, chicory, kiwi fruit, lettuce, mint, mustard greens, olive oil, parsley, peas, pistachios, red seaweed, spinach greens, spring onions, soybeans, tea leaves (but not tea drink), turnip greens, watercress.
Why is this necessary?
If you have suffered deep vein thrombosis of the lower or upper extremities, your doctor will most likely prescribe you indirect anticoagulants.
The main drug in this group today, both here and abroad, is warfarin. In our country, another drug of this group is used quite widely - phenylin. Other coumarin drugs (acenocoumarol, marcumar, marivan) can be used. The recommendations given are mostly applicable to any anticoagulant. The purpose of this medication is to prevent blood clots from recurring, which could cause your condition to worsen or cause life-threatening complications. The risk of recurrence of thrombosis is quite high during the first year after the first episode of the disease, therefore, taking into account various factors, warfarin is prescribed for a period of 2 to 12 months. In rare cases, longer therapy is performed. Indirect anticoagulants have no effect on an already formed blood clot.
To determine the duration of treatment, special (including genetic) blood tests are sometimes required to identify an increased tendency to blood clots.
A very large number of patients around the world receive the treatment you have prescribed. It is used not only in phlebology, but also in such areas of medicine as vascular surgery. In addition to deep vein thrombosis, the basis for prescribing anticoagulant therapy is often previous heart attacks, cardiac arrhythmias, valve and peripheral vessel replacement, and much more.
Other indirect anticoagulants[edit | edit code]
Dicumarol[edit | edit code]
This is the first indirect anticoagulant that was isolated and introduced into clinical practice. Today it is rarely used due to poor and unpredictable absorption and a high risk of gastrointestinal side effects. The maintenance dose of dicumarol is usually 25-200 mg/day. The effect appears within 1-5 days and after withdrawal continues for another 2-10 days. phenprocoumon and acenocoumarol. These funds are used primarily outside the United States. Phenprocoumon has a longer T1/2 (5 days) than warfarin, a slightly delayed onset and a longer duration of action (7-14 days). The maintenance dose is 0.75-6 mg/day. On the contrary, acenocoumarol has a short half-life (10-24 hours), rapid onset and short duration of action (2 days). Its maintenance dose is 1-8 mg/day.
Indandione derivatives[edit | edit code]
Anisindione is approved for use in the USA. It is similar in pharmacokinetics to warfarin, but has no apparent advantages and is more likely to cause side effects. Phenindione was very popular at one time, and is still used in some countries. However, due to the threat of severe, sometimes fatal allergic reactions that occur in the first weeks of treatment, its use is not recommended.
Rodenticides[edit | edit code]
Bromadiolone, brodifacoum, diphenadione, chlorphasinone and pindon are long-acting agents (prolongation of PT is observed over several weeks). They are of medical interest due to the possibility of accidental or intentional poisoning.
Monitoring the dose of warfarin
If the dose of the drug is selected, less frequent monitoring is sufficient - first once every 2 weeks, then once a month. The frequency of additional studies is determined separately. The need for an extraordinary determination of the INR may arise in a number of cases, which we will discuss below. If in any doubt, ask your doctor for advice.
Currently, there are portable devices for self-determination of INR (similar to systems for monitoring blood sugar levels in patients with diabetes), but their cost is very high and, in most cases of deep vein thrombosis, purchasing them is impractical.
Content
- 1 Warfarin 1.1 Historical background
- 1.2 Chemical structure
- 1.3 Pharmacological properties 1.3.1 Mechanism of action
- 1.3.2 Doses
- 1.3.3 Suction
- 1.3.4 Distribution
- 1.3.5 Elimination
- 1.3.6 Drug interactions
- 1.3.7 Warfarin resistance
- 1.3.8 Side effects
- 3.1 Dicumarol
Warfarin dose selection
The most difficult and responsible stage. “Loading” initial doses of warfarin (more than 5 mg) are not recommended.
Dose selection can be carried out both with and without the use of low molecular weight heparins (Fraxiparine, Clexane), both in the hospital and on an outpatient basis. The selection period on average takes from 1 to 2 weeks, but in some cases it increases to 2 months. At this time, you will need frequent INR determinations, up to 2 - 3 times a week or daily. Each time, after receiving the next test result, your doctor will determine a change in the dose of the medication and the date of the next test.
If in several tests in a row the INR remains in the range of 2.0 - 2.5, this means that the dose of warfarin has been adjusted. Further monitoring of treatment will be much easier.
Overdose of the drug Warfarin nycomed, symptoms and treatment
The optimal therapeutic effect of the drug is on the verge of bleeding, so microhematuria, bleeding gums, etc. are possible. If the patient does not have diseases that can provoke bleeding (for example, urolithiasis), such bleeding does not pose a serious danger as long as the prothrombin time exceeds 5%. In case of minor bleeding, it is enough to reduce the dose of the drug or interrupt treatment for a while. In case of serious bleeding, vitamin K is prescribed intravenously as an antidote at a dose of 5–10 mg. In case of life-threatening bleeding, immediate transfusion of prothrombin complex factor concentrate or fresh frozen blood plasma or whole blood is necessary.
How to monitor treatment
Carrying out antithrombotic (anticoagulant) therapy can save your life and health, but requires increased attention and mandatory compliance with the doctor’s recommendations. Warfarin is a drug that reduces the ability of blood to clot, so its excess can lead to hemorrhagic complications, i.e. to bleeding. To avoid complications, the required dose of warfarin is monitored using a blood test called INR (International Normalized Ratio). This may sometimes be referred to as INR in laboratory responses. During the entire period of taking warfarin, the INR should be in the range of 2.0 - 3.0. If the INR is less than 2.0, then blood clotting is not reduced and thrombotic complications are possible. If the INR is more than 4.0, hemorrhagic complications are very real. An increase in INR from 2.5 to 4.0 indicates the need to reduce the dose of the drug, but usually does not pose a direct threat. For some diseases, the required upper limit of INR is 4.0 - 4.4.
In the absence of the ability to determine INR, monitoring by prothrombin time (PT) is acceptable, but this method is much less reliable. No other blood tests are needed to calculate your warfarin dose. To identify the side effects of the drug, a general blood test, urine test and some biochemical tests are periodically prescribed.
How to take the drug
Warfarin is available in 2.5 milligram tablets. Most often, the “starting” and “maintenance” doses of the drug are 5 milligrams (2 tablets) per day. In many cases, for more “fine” adjustments, you will change the dose of the medicine that you take not per day, but per week. This may require either dividing the tablet in half or taking different numbers of tablets on different days. To make it easier to monitor your treatment, you may be given a special account book, or you can keep a notebook with a treatment diary, where it is useful to note the doses of warfarin, INR level, and other laboratory data.
Warfarin is taken in the entire daily dose at one time, preferably at 17:00 - 19:00. Take the tablets with water. It is not recommended to take it with food, but can be taken on an empty stomach. Phenyline is usually taken in 2 doses.