Artificial respiration (AR) is an urgent emergency measure if a person’s own breathing is absent or impaired to such an extent that it poses a threat to life. The need for artificial respiration may arise when providing assistance to those who have received sunstroke, drowned, suffered from electric current, as well as in case of poisoning with certain substances.
The purpose of the procedure is to ensure the process of gas exchange in the human body, in other words, to ensure sufficient saturation of the victim’s blood with oxygen and the removal of carbon dioxide from it. In addition, artificial ventilation has a reflex effect on the respiratory center located in the brain, as a result of which independent breathing is restored.
Mechanism and methods of artificial respiration
Content:
- Mechanism and methods of artificial respiration
- Indications and contraindications
- Preparing for artificial respiration
- Artificial respiration from mouth to mouth
- Artificial respiration from mouth to nose
- How long does artificial respiration last?
- Features of the procedure in children
- Manual methods of artificial respiration
- Hardware artificial respiration methods
- Complications of artificial respiration
Only through the process of breathing does a person’s blood become saturated with oxygen and carbon dioxide is removed from it. After air enters the lungs, it fills the lung sacs called alveoli. The alveoli are pierced by an incredible number of small blood vessels. It is in the pulmonary vesicles that gas exchange takes place - oxygen from the air enters the blood, and carbon dioxide is removed from the blood.
If the body's supply of oxygen is interrupted, vital activity is at risk, since oxygen plays the “first fiddle” in all oxidative processes that occur in the body. That is why, when breathing stops, artificially ventilating the lungs should be started immediately.
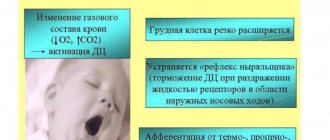
The air entering the human body during artificial respiration fills the lungs and irritates the nerve endings in them. As a result, nerve impulses are sent to the respiratory center of the brain, which are a stimulus for the production of response electrical impulses. The latter stimulate contraction and relaxation of the diaphragm muscles, resulting in stimulation of the respiratory process.
Artificially supplying the human body with oxygen in many cases makes it possible to completely restore the independent respiratory process. In the event that cardiac arrest is also observed in the absence of breathing, it is necessary to perform a closed cardiac massage.
Please note that the absence of breathing triggers irreversible processes in the body within five to six minutes. Therefore, timely artificial ventilation can save a person’s life.
All methods of performing ID are divided into expiratory (mouth-to-mouth and mouth-to-nose), manual and hardware. Manual and expiratory methods are considered more labor-intensive and less effective compared to hardware methods. However, they have one very significant advantage. They can be performed without delay, almost anyone can cope with this task, and most importantly, there is no need for any additional devices and instruments, which are not always at hand.
When is mechanical ventilation required?
Mechanical ventilation is used to provide assistance in cases where the patient is unable to independently inhale the amount of oxygen necessary for the full functioning of the body, as well as exhale carbon dioxide. The need for mechanical ventilation arises in the absence of natural breathing or when it is seriously impaired, for example, due to injuries, as well as during surgical procedures under anesthesia.
It is important to understand that timely connection of the patient to a ventilator maximizes his chances of survival. If a person who has stopped breathing is not connected to a ventilator, his internal organs are no longer supplied with oxygen. Afterwards, the heart stops, and hence the blood supply to the entire body, and the patient dies within a couple of minutes.
Ventilators are the most common format for artificial ventilation of the lungs
Indications and contraindications
Indications for the use of ID are all cases where the volume of spontaneous ventilation of the lungs is too low to ensure normal gas exchange. This can happen in many urgent and planned situations:
- For disorders of the central regulation of breathing caused by impaired cerebral circulation, tumor processes of the brain or brain injury.
- For medicinal and other types of intoxication.
- In case of damage to the nerve pathways and neuromuscular synapse, which can be caused by trauma to the cervical spine, viral infections, the toxic effect of certain medications, and poisoning.
- For diseases and damage to the respiratory muscles and chest wall.
- In cases of lung lesions of both obstructive and restrictive nature.
The need to use artificial respiration is judged based on a combination of clinical symptoms and external data. Changes in pupil size, hypoventilation, tachy- and bradysystole are conditions that require artificial ventilation. In addition, artificial respiration is required in cases where spontaneous ventilation is “turned off” with the help of muscle relaxants administered for medical purposes (for example, during anesthesia for surgery or during intensive care for a seizure disorder).
As for cases where ID is not recommended, there are no absolute contraindications. There are only prohibitions on the use of certain methods of artificial respiration in a particular case. So, for example, if venous return of blood is difficult, artificial respiration modes are contraindicated, which provoke even greater disruption. In case of lung injury, ventilation methods based on high-pressure air injection, etc., are prohibited.
Non-invasive pulmonary ventilation (NIV) - what is it?
This method of artificial pulmonary ventilation is indicated for patients without bulbar disorders. It is a non-invasive option for respiratory support using a ventilator. In other words, through a mask, special nasal cannulas, and a mouthpiece.
NIV has its advantages. They consist in the fact that all the functions of the natural respiratory tract are preserved, and there is no need for surgical intervention. This reduces the number of possible complications and side effects.
The key to successful use of noninvasive ventilation is understanding both its benefits and limitations. Careful selection of patients is also necessary (clarification of the diagnosis, assessment of the condition, further treatment plan). Indications for NIV include the following criteria:
- shortness of breath at rest;
- respiratory rate (RR)>25, participation of auxiliary respiratory muscles in the respiratory process;
- hypercapnia (PaC02>45 and its rapid increase);
- Ph level <7.35 and its rapid decline;
- symptomatic lack of positive effect from oxygen therapy, hypoxemia and gas exchange disorders;
- increase in airway resistance by 1.5-2 times the norm.
The NIV technique is the most comfortable and safe for the patient
Preparing for artificial respiration
Before performing expiratory artificial respiration, the patient should be examined. Such resuscitation measures are contraindicated for facial injuries, tuberculosis, poliomelitis and trichlorethylene poisoning. In the first case, the reason is obvious, and in the last three, performing expiratory artificial respiration puts the person performing resuscitation at risk.
Before starting expiratory artificial respiration, the victim is quickly freed from clothing squeezing the throat and chest. The collar is unbuttoned, the tie is undone, and the trouser belt can be unfastened. The victim is placed supine on his back on a horizontal surface. The head is tilted back as much as possible, the palm of one hand is placed under the back of the head, and the other palm is pressed on the forehead until the chin is in line with the neck. This condition is necessary for successful resuscitation, since with this position of the head the mouth opens and the tongue moves away from the entrance to the larynx, as a result of which air begins to flow freely into the lungs. In order for the head to remain in this position, a cushion of folded clothing is placed under the shoulder blades.
After this, it is necessary to examine the victim’s oral cavity with your fingers, remove blood, mucus, dirt and any foreign objects.
It is the hygienic aspect of performing expiratory artificial respiration that is the most delicate, since the rescuer will have to touch the victim’s skin with his lips. You can use the following technique: make a small hole in the middle of a handkerchief or gauze. Its diameter should be two to three centimeters. The fabric is placed with a hole on the victim’s mouth or nose, depending on which method of artificial respiration will be used. Thus, air will be blown through the hole in the fabric.
Classification
Ventilators are usually classified depending on a number of parameters:
- According to the patient’s age: there are different options for children over 6 years old and adults, for children under 6 years old, for infants and newborns;
- By mode of action: external, internal, electrical stimulators;
- By type of drive: manual, electric, pneumatic;
- By purpose: stationary or transport (they are also called mobile).
Do I need to buy oxygen tanks? More details
Artificial respiration from mouth to mouth
To perform artificial respiration using the mouth-to-mouth method, the person who will provide assistance must be on the side of the victim’s head (preferably on the left side). In a situation where the patient is lying on the floor, the rescuer kneels. If the victim's jaws are clenched, they are forced apart.
After this, one hand is placed on the victim’s forehead, and the other is placed under the back of the head, tilting the patient’s head back as much as possible. Having taken a deep breath, the rescuer holds the exhalation and, bending over the victim, covers the area of his mouth with his lips, creating a kind of “dome” over the patient’s mouth. At the same time, the victim’s nostrils are pinched with the thumb and index finger of the hand located on his forehead. Ensuring tightness is one of the prerequisites for artificial respiration, since air leakage through the victim’s nose or mouth can nullify all efforts.
After sealing, the rescuer quickly, forcefully exhales, blowing air into the airways and lungs. The duration of exhalation should be about a second, and its volume should be at least a liter for effective stimulation of the respiratory center to occur. At the same time, the chest of the person receiving assistance should rise. If the amplitude of its rise is small, this is evidence that the volume of air supplied is insufficient.
Exhaling, the rescuer unbends, freeing the victim's mouth, but at the same time keeping his head thrown back. The patient should exhale for about two seconds. During this time, before taking the next breath, the rescuer must take at least one normal breath “for himself.”
Please note that if a large amount of air enters the patient's stomach rather than the lungs, this will significantly complicate his rescue. Therefore, you should periodically press on the epigastric region to empty the stomach of air.
Artificial respiration from mouth to nose
This method of artificial ventilation is carried out if it is not possible to properly unclench the patient’s jaws or there is an injury to the lips or oral area.
The rescuer places one hand on the victim’s forehead and the other on his chin. At the same time, he simultaneously throws back his head and presses his upper jaw to the lower. With the fingers of the hand that supports the chin, the rescuer must press the lower lip so that the victim’s mouth is completely closed. Taking a deep breath, the rescuer covers the victim’s nose with his lips and forcefully blows air through the nostrils, while watching the movement of the chest.
After artificial inspiration is completed, you need to free the patient's nose and mouth. In some cases, the soft palate may prevent air from escaping through the nostrils, so when the mouth is closed, there may be no exhalation at all. When exhaling, the head must be kept tilted back. The duration of artificial exhalation is about two seconds. During this time, the rescuer himself must take several exhalations and inhalations “for himself.”
How long does artificial respiration last?
There is only one answer to the question of how long ID should be carried out. You should ventilate your lungs in this mode, taking breaks for a maximum of three to four seconds, until full spontaneous breathing is restored, or until the doctor appears and gives other instructions.
At the same time, you should constantly ensure that the procedure is effective. The patient's chest should swell well, and the facial skin should gradually turn pink. It is also necessary to ensure that there are no foreign objects or vomit in the victim’s respiratory tract.
Please note that due to the ID, the rescuer himself may experience weakness and dizziness due to a lack of carbon dioxide in the body. Therefore, ideally, air blowing should be done by two people, who can alternate every two to three minutes. If this is not possible, the number of breaths should be reduced every three minutes so that the person performing resuscitation normalizes the level of carbon dioxide in the body.
During artificial respiration, you should check every minute to see if the victim’s heart has stopped. To do this, use two fingers to feel the pulse in the neck in the triangle between the windpipe and the sternocleidomastoid muscle. Two fingers are placed on the lateral surface of the laryngeal cartilage, after which they are allowed to “slide” into the hollow between the sternocleidomastoid muscle and the cartilage. This is where the pulsation of the carotid artery should be felt.
If there is no pulsation in the carotid artery, chest compressions in combination with ID should be started immediately. Doctors warn that if you miss the moment of cardiac arrest and continue to perform artificial ventilation, it will not be possible to save the victim.
How do ventilators work?
Modern ventilators are high-tech, “intelligent” medical equipment. They provide respiratory support to the patient both in volume and pressure, which is fundamentally important for restoring normal functioning of the body.
The principle by which ventilators operate is called positive pressure ventilation. They pump oxygen-rich air into the lungs and pump fluid out of them. The devices have many different ventilation modes, which are used depending on the specific situation and are individually selected for each patient.
With Pressure Controlled Ventilation (PCV), the device creates an optimal level of oxygen in the alveoli and airways, which allows the lungs to absorb as much oxygen as possible. As soon as the pressure reaches the set maximum limit, the exhalation mode begins. Thus, the equipment takes over the entire breathing process of the patient.
One of the most advanced technologies for synchronizing the ventilator with the patient is neuro-controlled ventilation. In this case, the signal coming from the respiratory center of the human medulla oblongata along the phrenic nerve to the diaphragm is recorded by special highly sensitive sensors located in the area of the transition of the esophagus to the stomach (cardia).
Any device must have the ability to dose oxygen and control carbon dioxide in the exhaled air.
There are both invasive and non-invasive methods of artificial lung ventilation
Features of the procedure in children
When performing artificial ventilation for babies under one year of age, the mouth-to-mouth and nose technique is used. If the child is older than one year, the mouth-to-mouth method is used.
Small patients are also placed on their back. For babies under one year old, place a folded blanket under their back or slightly raise their upper body, placing a hand under their back. The head is thrown back.
The person providing assistance takes a shallow breath, seals her lips around the child’s mouth and nose (if the baby is under one year old) or just the mouth, and then blows air into the respiratory tract. The volume of air blown in should be less, the younger the patient. So, in the case of resuscitation of a newborn, it is only 30-40 ml.
If a sufficient volume of air enters the respiratory tract, chest movement occurs. After inhaling, you need to make sure that the chest drops. If you blow too much air into your baby's lungs, this can cause the alveoli of the lung tissue to rupture, causing air to escape into the pleural cavity.
The frequency of insufflations should correspond to the breathing frequency, which tends to decrease with age. Thus, in newborns and children up to four months, the frequency of inhalations and exhalations is forty per minute. From four months to six months this figure is 40-35. In the period from seven months to two years - 35-30. From two to four years it is reduced to twenty-five, in the period from six to twelve years - to twenty. Finally, in a teenager aged 12 to 15 years, the respiratory rate is 20-18 breaths per minute.
Manual methods of artificial respiration
There are also so-called manual methods of artificial respiration. They are based on changing the volume of the chest due to the application of external force. Let's look at the main ones.
Sylvester's method
This method is most widely used. The victim is placed on his back. A cushion should be placed under the lower part of the chest so that the shoulder blades and the back of the head are lower than the costal arches. In the event that artificial respiration is performed using this method by two people, they kneel on either side of the victim so as to be positioned at the level of his chest. Each of them holds the victim’s hand in the middle of the shoulder with one hand, and with the other just above the level of the hand. Next, they begin to rhythmically raise the victim’s arms, stretching them behind his head. As a result, the chest expands, which corresponds to inhalation. After two or three seconds, the victim’s hands are pressed to the chest, while squeezing it. This performs the functions of exhalation.
In this case, the main thing is that the movements of the hands are as rhythmic as possible. Experts recommend that those performing artificial respiration use their own rhythm of inhalation and exhalation as a “metronome”. In total, you should do about sixteen movements per minute.
ID using the Sylvester method can be performed by one person. He needs to kneel behind the victim’s head, grab his arms above the hands and perform the movements described above.
For broken arms and ribs, this method is contraindicated.
Schaeffer method
If the victim's arms are injured, the Schaeffer method can be used to perform artificial respiration. This technique is also often used for the rehabilitation of people injured while on the water. The victim is placed prone, with his head turned to the side. The one who performs artificial respiration kneels, and the victim’s body should be located between his legs. Hands should be placed on the lower part of the chest so that the thumbs lie along the spine and the rest rest on the ribs. When exhaling, you should lean forward, thus compressing the chest, and while inhaling, straighten, stopping the pressure. The elbows are not bent.
Please note that this method is contraindicated for fractured ribs.
Laborde method
The Laborde method is complementary to the Sylvester and Schaeffer methods. The victim's tongue is grabbed and rhythmically stretched, imitating breathing movements. As a rule, this method is used when breathing has just stopped. The resistance of the tongue that appears is evidence that the person’s breathing is being restored.
Kallistov method
This simple and effective method provides excellent ventilation. The victim is placed prone, face down. A towel is placed on the back in the area of the shoulder blades, and its ends are passed forward, threaded under the armpits. The person providing assistance should take the towel by the ends and lift the victim’s torso seven to ten centimeters from the ground. As a result, the chest expands and the ribs rise. This corresponds to inhalation. When the torso is lowered, it simulates exhalation. Instead of a towel, you can use any belt, scarf, etc.
Howard's method
The victim is positioned supine. A cushion is placed under his back. Hands are moved behind the head and extended. The head itself is turned to the side, the tongue is extended and secured. The one who performs artificial respiration sits astride the victim’s thigh area and places his palms on the lower part of the chest. With your fingers spread, you should grab as many ribs as possible. When the chest is compressed, it simulates inhalation; when the pressure is released, it simulates exhalation. You should do twelve to sixteen movements per minute.
Frank Eve's method
This method requires a stretcher. They are installed in the middle on a transverse stand, the height of which should be half the length of the stretcher. The victim is placed prone on the stretcher, the face is turned to the side, and the arms are placed along the body. The person is tied to the stretcher at the level of the buttocks or thighs. When lowering the head end of the stretcher, inhale; when it goes up, exhale. Maximum breathing volume is achieved when the victim's body is tilted at an angle of 50 degrees.
Nielsen method
The victim is placed face down. His arms are bent at the elbows and crossed, after which they are placed palms down under the forehead. The rescuer kneels at the victim’s head. He places his hands on the victim’s shoulder blades and, without bending them at the elbows, presses with his palms. This is how exhalation occurs. To inhale, the rescuer takes the victim’s shoulders at the elbows and straightens, lifting and pulling the victim towards himself.
Hardware artificial respiration methods
For the first time, hardware methods of artificial respiration began to be used back in the eighteenth century. Even then, the first air ducts and masks appeared. In particular, doctors proposed using fireplace bellows to blow air into the lungs, as well as devices created in their likeness.
The first automatic ID machines appeared at the end of the nineteenth century. At the beginning of the twenties, several types of respirators appeared at once, which created intermittent vacuum and positive pressure either around the entire body, or only around the patient’s chest and abdomen. Gradually, respirators of this type were replaced by air-injection respirators, which had less solid dimensions and did not impede access to the patient’s body, allowing medical procedures to be performed.
Best materials of the month
- Coronaviruses: SARS-CoV-2 (COVID-19)
- Antibiotics for the prevention and treatment of COVID-19: how effective are they?
- The most common "office" diseases
- Does vodka kill coronavirus?
- How to stay alive on our roads?
All ID devices existing today are divided into external and internal. External devices create negative pressure either around the patient's entire body or around his chest, thereby inhaling. Exhalation in this case is passive - the chest simply collapses due to its elasticity. It can also be active if the device creates a positive pressure zone.
With the internal method of artificial ventilation, the device is connected through a mask or intubator to the respiratory tract, and inhalation is carried out by creating positive pressure in the device. Devices of this type are divided into portable, intended for work in “field” conditions, and stationary, the purpose of which is long-term artificial respiration. The former are usually manual, while the latter operate automatically, driven by a motor.
Risks of use
It is worth understanding that the use of a ventilator is an emergency option when it is impossible to save a person’s life in any other way. However, there are certain risks when using such a device. And it’s worth knowing about them so that there are no unpleasant surprises.
Article on the topic
The pathologist speaks. What happens to organs after infection with COVID-19? All complications that may be associated with the use of the device are divided into two groups: early and late. The first develop immediately, within a few hours from the moment of connection. Others will be delayed and may appear even after a few weeks.
For example, problems with hemodynamics may arise. This usually happens in those whose blood volume decreases, because when the device is operating, changes in pressure and its outflow and inflow begin. As a rule, this condition does not require any special serious correction.
If a person has pulmonary pathologies, for example, bullous emphysema, pneumosclerosis, destructive pneumonia, barotrauma may occur.
Tracheal stenosis after intubation is one of the late complications. Usually manifests as difficulty breathing. Among the delayed effects, one can also distinguish sinusitis, which can develop against the background of prolonged intubation. Doctors usually see a general inflammatory response. They are diagnosed using x-rays. This type of complication is treated with antibiotics, selected exclusively by a doctor, depending on the severity of the situation and the severity of the symptoms.
Another option is tracheobronchitis. It most often manifests itself on the second or third day, less often on the third or fifth. In mild cases, there are complaints of a foreign body sensation, a feeling of fullness, and pain. The amount of sputum also increases.
Death from a runny nose. What dangerous complications are fraught with ENT diseases? More details