Pharmacological properties of the drug Glibenclamide
Oral antidiabetic agent, sulfonylurea derivative of the second generation. Glibenclamide has a hypoglycemic effect by stimulating the secretion of endogenous insulin by functioning β-cells of the islets of Langerhans of the pancreas and reducing the physiological threshold for stimulation of β-cells by glucose, as well as by increasing the sensitivity of insulin receptors in peripheral tissues to insulin and, presumably, enhancing the action of insulin at the post-receptor level . Has a hypolipidemic effect. When taken orally, glibenclamide is quickly and almost completely absorbed, the effect occurs after about 2 hours, the maximum hypoglycemic effect occurs 7–8 hours after oral administration, the duration of action is over 12 hours. The maximum concentration in blood plasma is achieved after 1–2 hours, period half-life is about 2–10 hours; more than 95% of the active substance is bound to plasma proteins. Glibenclamide is rapidly excreted from the body, almost completely metabolized in the liver, about 50% is excreted in the urine and about 50% in bile (including 4–6% unchanged).
Glibenclamide is a second-generation drug of sulfonylurea derivatives, the “gold standard” in the treatment of type 2 diabetes mellitus (T2DM). The drug has been used since 1969 as an effective remedy for the correction of hyperglycemia in T2DM in many countries around the world, and is a standard for assessing effectiveness when searching for new antidiabetic drugs in experimental studies and clinical practice [1].
Molecular mechanisms of action of glibenclamide
The targets of sulfonylurea derivatives are ATP-dependent potassium channels (K-ATP channels), which act as a regulator of β-cell membrane potential [2].
The K-ATP channel is a hetero-octamer complex consisting of two types of subunits: the potassium channel-forming subunit Kir6.x and the sulfonylurea receptor (SUR). SUR is a member of the ABC transporter family with 17 transmembrane helices comprising a group of 5 TMs, two repeats of 6 TMs, and a large cytosolic loop. The cytosolic loop of the receptor has two nucleotide-binding sites - NBF 1 and NBF 2, which specifically complex with Mg2+ and ADP/ATP. Four subunits of Kir6.x form a pore; binding of ATP to intracellular domains leads to channel inhibition [2–4]. There are several isoforms of both Kir6.x (Kir6.1, Kir6.2) and SUR (SUR1, SUR2A, SUR2B) subunits. In most tissues, Kir6.2 serves as a pore-forming subunit, but it is associated with various SUR subunits, for example, SUR1 in the pancreas and brain, SUR2A in the heart and skeletal muscle, and SUR2B in the brain and smooth muscle. The K-ATP channel in vascular smooth muscle consists of Kir6.1 and SUR2B subunits. Variations in the composition of the subunits of K-ATP channels cause differences in the metabolic and drug sensitivity of various organs and tissues to sulfonylurea derivatives [4, 5].
Sulfonylurea derivatives bind to the SUR-1 subunit of K-ATP channels, which leads to their closure, increased intracellular potassium concentration and depolarization of the β-cell membrane. In response to depolarization, calcium channels open, calcium concentration increases, which stimulates the migration and exocytosis of insulin granules [2].
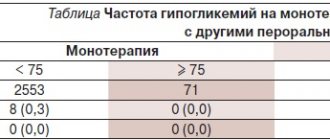
Differences in the effect of drugs on the insulin secretory function of the pancreas depend on the pharmacokinetics and affinity for various SUR subunits (see table).
Glibenclamide blocks K-ATP channels of pancreatic β-cells and cardiomyocytes, but the molecular mechanisms of action are not the same; for Kir6.2/SUR1 the inhibition can be irreversible, and for Kir6.2/SUR2A it is quickly reversible. The structure of glibenclamide contains tolbutamide and metheglinide motifs, which explains the binding to SUR1 at two sites, and SUR2A at only one benzamide site. In addition, inhibition of Kir6.2/SUR1 is irreversible, since simultaneous dissociation of the receptor-junction complex will occur with a lower probability. This may explain the long washout period in studies after discontinuation of glibenclamide in patients with diabetes [5, 6].
Efficacy and safety of the drug
Sulfonylureas, along with metformin, are considered one of the most effective classes of oral hypoglycemic drugs. With rational pharmacotherapy of T2DM, drugs can reduce the level of glycosylated hemoglobin by 1-2%, which significantly reduces the risk of developing late complications [7].
However, when treating T2DM, it is necessary to remember the risk of developing hypoglycemic conditions.
In the UKPDS study, 31% of patients experienced mild hypoglycemia during the 1st year of treatment with glibenclamide; severe hypoglycemia with sulfonylurea therapy was observed in 1% [8]. The risk of hypoglycemic conditions is associated with the fact that glibenclamide has the highest affinity for K-ATP channels of pancreatic β-cells among sulfonylurea derivatives [6]. In addition, it should be noted that the risk of hypoglycemia increases in elderly patients, with moderate hyperglycemia, irregular diet, and alcohol consumption [8].
Although sulfonylureas are effective oral hypoglycemic agents, there is interindividual variability in response to the drug. The ADOPT (Diabetes Outcome Progression Trial) studies showed that failure of monotherapy with glibenclamide after 5 years was 34%, rosiglitazone - 15% and metformin - 32%. Clinical factors such as decreased β-cell function, high baseline glucose levels, and insulin resistance are predictive of monotherapy failure [9].
Polymorphisms in drug target genes (ABCC8, KCNJ11) and diabetes risk genes (TCF7L2, IRS-1) were found to be associated with variability in response to sulfonylureas in patients with T2DM. Thus, the E23K variant of KCNJ11 is associated with an increased risk of secondary resistance in patients on sulfonylurea therapy. When studied ex vivo
the influence of the E23K genotype on the physiological activity of human pancreatic islets, it was revealed that in the islets of allele carriers, after administration of sulfonylurea derivatives, insulin secretory function was statistically insignificantly reduced, however, subsequent 24-hour exposure to glucose in high concentrations significantly reduced glibenclamide-induced insulin secretion. The ABCC8 Ser1369Ala polymorphism is associated with differences in response to therapy with sulfonylurea derivatives; in clinical studies, carriers of the allele have a more significant decrease in glucose and glycosylated hemoglobin levels [10].
Thus, the new ADA-EASD approach (2012) is justified, based on the personalization of T2DM therapy and taking into account the pathogenesis of the disease, the patient’s lifestyle, comorbidities and treatment costs.
Micronized form of glibenclamide
According to the Biopharmaceutics Drug Classification System, glibenclamide belongs to class II drugs [11]. Crystalline glibenclamide, produced in various countries, has a maximum dissolution of more than 40% [12]. The solubility of glibenclamide in gastric juice and the pH in the gastrointestinal tract affect the absorption of the drug [11]. Comparative post-marketing studies of glibenclamide have demonstrated variations in bioavailability and dosage form dependence of oral absorption [13]. To increase the solubility and bioavailability of glibenclamide, various approaches have been used, which included the addition of surfactants, the formation of complexes with cyclodextrins, the preparation of solid dispersion systems, micronization and transformation of the crystal lattice of the compound [11, 14]. The solubility of a drug is related to the size of its particles: during micronization, a decrease in particle size and an increase in surface area increases solubility, thereby increasing adsorption in the gastrointestinal tract, bioavailability and clinical effectiveness of the drug [14].
Micronisironization of glibenclamide increased the rate of absorption (by 50%) and the postprandial effect, increased bioavailability, which made it possible to use the drug in lower doses and reduce the risk of hypoglycemic conditions [15]. A comparison of the efficacy and safety of non-micronized (5 mg) and micronized (3 mg) forms of glibenclamide was conducted in a 12-week randomized, double-blind study, which demonstrated no differences in the level of glycosylated hemoglobin, C-peptide, and postprandial glucose concentrations [16].
Cardiovascular risk
The question of the cardiovascular safety of sulfonylurea derivatives first arose in 1970 with reports that tolbutamide increased mortality from cardiovascular pathology compared with insulin therapy [17]. A possible reason for this fact is that K-ATP channels regulated by the SUR subunit are localized in cardiomyocytes and vascular smooth muscles [18]. Sulfonylurea derivatives, by blocking channels, have a negative effect on three processes in the myocardium: relaxation of vascular smooth muscles, which improves coronary blood flow, limitation of myocardial damage during ischemia, and protection of cardiomyocyte mitochondria [17, 18]. The presence of K-ATP channels in the myocardium is one of the important mechanisms underlying the phenomenon of ischemic preconditioning. The cardioprotective effect of ischemic preconditioning is expressed in reducing the size of the infarction, improving the mechanical function of the heart, and reducing the frequency of ventricular arrhythmia against the background of ischemia, which without the implementation of this phenomenon would lead to much more serious clinical consequences or even death [18].
Thus, sulfonylurea derivatives specific not only to the SUR subunit of the K-ATP channel of β-cells, but also to cardiomyocytes, can reduce coronary blood flow and prevent ischemic preconditioning [19, 20].
M. Loubania et al. [21] conducted studies to study the effect of glibenclamide and gliclazide on ischemic preconditioning and the effect of glibenclamide on signal transduction in the myocardium in areas of the right atrium of patients obtained after heart surgery. The cardioprotective effect of ischemic preconditioning was leveled by glibenclamide in the concentration range of 0.1-10 µmol/l, and gliclazide in supratherapeutic concentrations (10, 100 µmol/l). It should be noted that glibenclamide inhibited the protective effect associated with the opening of K-ATP channels, but did not affect the activation of protein kinase C and p38 mitogen-activated protein kinase during ischemic preconditioning.
However, data from clinical studies on the cardiovascular safety of sulfonylurea derivatives, in particular glibenclamide, are contradictory.
Retrospective cohort studies [22] provided evidence of an increase in mortality after myocardial infarction (MI) in a group of patients receiving sulfonylurea monotherapy, but an increased risk of mortality was associated with the use of high doses of glibenclamide. Retrospective cohort studies [23] found that the use of high doses of sulfonylurea derivatives increases the risk of heart failure compared with metformin. In patients with T2DM who were treated with high doses of sulfonylurea derivatives (average daily dose of glibenclamide more than 4 mg), the likelihood of developing heart failure (relative risk 1.20-1.60) is higher than in patients receiving low doses of drugs. The use of sulfonylureas increased in-hospital mortality in patients undergoing coronary balloon angioplasty after MI [24]. T. Schramm et al. [25] summarized data from a nationwide study assessing mortality and cardiovascular risk associated with the use of sulfonylureas and metformin in patients with T2DM. A total of 107,806 patients were included in the study, of whom 9,607 suffered an acute MI. Compared with metformin, glibenclamide increased overall mortality (relative risk 1.24–1.40) and cardiovascular mortality (relative risk 1.03–1.25) in patients without prior MI. Corresponding results were obtained when analyzing a group of patients with T2DM and previous MI. It should be noted that during therapy with glimepiride and glipizide, similar data were observed on overall mortality and mortality from cardiovascular pathology.
The UKPDS study [17] conducted a comparative analysis of the effectiveness and safety of metformin, chlorpropamide, glibenclamide and insulin. The study revealed no differences in mortality and risks of MI with different treatment regimens. In the prospective LAMBDA study, prior glibenclamide therapy did not have a negative effect on survival in patients with MI [26]. In the ADOPT trial [9], the rate of cardiovascular events was lower with glibenclamide than with rosiglitazone or metformin (1.8, 3.4 and 3.2%, respectively). This effect is mainly due to fewer cases of congestive heart failure and a lower incidence of non-fatal myocardial infarction in the glibenclamide-treated group.
Systematic review by E. Selvin et al. [27] studied the degree of cardiovascular risk during treatment of diabetes with oral antidiabetic drugs and summarized data from 40 controlled studies that recorded cardiovascular events (mainly MI and stroke) in patients with type 2 diabetes receiving second-generation sulfonylureas, biguanides, thiazolidinediones or meglitinides. An analysis of clinical studies did not reveal an association between the use of glucose-lowering drugs and an increase in the incidence of fatal and non-fatal cardiovascular events, as well as overall mortality.
Outlook: neuroprotective effect (data from experimental studies and prospective clinical trials)
A second potential role for K-ATP channels that needs to be considered is their involvement in neuroprotection. Neuronal K-ATP channels are activated under metabolic conditions that deplete ATP, such as hypoxia. Sulfonylureas may reduce hypoxia-induced hyperpolarization in hippocampal and neocortical neurons, thereby counteracting the neuroprotective function of these channels. However, it is believed that K-ATP channels perform a protective function only under strictly limited conditions of hypoxia, in conditions that are accompanied by depletion of ATP synthesis and the development of energy deficiency, which leads to dysfunction of active transport channels, destabilization of cell membranes, release of neurotransmitters and irreversible damage neurons [28]. It should be noted that SUR1, in addition to the K-ATP channel, associates with the calcium-sensitive non-selective cation channel (NCCa-ATP) and forms the SUR1-NCCa-ATP channel, therefore, data on potential negative effects when using sulfonylurea derivatives to regulate the NCCa-ATP function must be taken into account . The SUR1-regulated NCCa-ATP channel is not constitutively expressed; the number of channels increases in the CNS under conditions of hypoxia and injury [29].
The channel transports monovalent cations (Na+, K+, Cs+, Li+, Rb+), equivalent in size to the pore radius of 0.41 nm, and is impermeable to Ca2+ and Mg2+. Channel opening requires physiological concentrations of calcium on the cytoplasmic side and is blocked by intracellular ATP (effective dose 50 (EC 50) - 0.79 mmol/l), but not ADP and AMP. The primary function of Sur1-NCCa-ATP channels is to protect against pathological increases in calcium levels, one of the hallmarks of CNS damage, but the channels are also activated by intracellular ATP depletion, which occurs in stroke and traumatic brain injury. Uncontrolled opening of channels, which in turn leads to an increase in the flow of sodium and water into the cell, ends with cell swelling, the formation of large fluid bubbles, oncotic necrosis and cell death. This pathological mechanism involving Sur1-NCCa-ATP channels is activated in most CNS injuries, including stroke and traumatic injuries to the brain and spinal cord, and subarachnoid hemorrhages [28, 29].
Studies on glial astrocytes have demonstrated that the channel is blocked by sulfonylurea derivatives of the first (tolbutamide, EC50, 16.1 mmol/L at pH 7.4) and second (glibenclamide, EC50, 48 nmol/L at pH 7.4) generations. The effect of sulfonylurea derivatives on the Sur1-NCCa-ATP channel is associated with a prolongation and increase in the time the channel is in the closed state; the drugs do not have an effect on the time the channel is open and conductivity [30]. In addition, the blocking activity of glibenclamide increases with decreasing pH values [29, 30].
Pharmacological inhibition of the SUR1 subunit with glibenclamide within 3 hours after injury protects capillaries, prevents fragmentation of capillary walls, inhibits the progression of hemorrhagic necrosis and stops the spread of hemorrhagic contusion on the contralateral side in traumatic spinal cord injury. The results of this study were confirmed in 4 separate series of experiments on rats, in addition to the above effects, improvements in neurological function were observed [29]. In addition, the effectiveness of the use of glibenclamide in low doses (below therapeutic) in traumatic brain injury has been proven [31]. A prospective, multicenter, placebo-controlled, Phase IIa clinical trial of RPF-1127 (an injectable form of glibenclamide) is testing the drug's efficacy in patients with traumatic brain injury.
J. Simard et al. [32] examined the effects of low doses of glibenclamide in 3 ischemic models. Glibenclamide reduced the total volume of damage by 53% in thromboembolic ischemia, reduced the volume of cortical damage by 51% in irreversible occlusion of the middle cerebral artery by filament, and by 41% the volume of cortical damage in temporary occlusion of the internal middle cerebral artery. The effectiveness of glibenclamide for CNS ischemia was assessed retrospectively in patients with T2DM with ischemic stroke. Subgroup analysis showed that sulfonylureas improved the NIHSS score (4 points or less) only in patients with nonlacunar stroke and further research is needed on the appropriateness of the use of drugs in ischemic stroke [33]. Another retrospective study [29] demonstrated that in a group of patients with T2DM treated with sulfonylurea derivatives, the risk of in-hospital mortality and worsening of neurological symptoms was reduced. A multicenter, prospective, open-label study of RP-1127 (GAMES-PILOT) is being conducted in patients with severe ischemic stroke with circulatory disorders.
The enormous importance of glibenclamide (micronized form, Maninil) for global diabetology was assessed at the annual medicine competition held by the Institute. G.G. Creutzfeldt (Kiel, Germany), awarded the HG Creutzfeldt Drug Prize in July 2010. The Expert Committee presented the following criteria for nomination: effectiveness confirmed by clinical practice over a long period of time; economic benefit, combines well with other drugs; reducing the risk of late complications; possibility of use in elderly patients and patients with multiple comorbidities; the presence of glibenclamide in the WHO list of essential medicines of the 16th revision (March 2010).
Special instructions for the use of the drug Glibenclamide
When treated with glibenclamide, the risk of developing hypoglycemia significantly increases in patients with impaired liver and kidney function, alcohol abuse, fasting or inadequately reduced carbohydrate intake, and excessive physical exercise. Taking beta-adrenergic blockers and drugs that act on the central nervous system may mask the symptoms of hypoglycemia. In elderly people, patients with atherosclerosis of cerebral vessels and senile dementia, the risk of developing hypoglycemia and its severity increase, and therefore it is preferable for them to prescribe glibenclamide in correspondingly reduced doses.
Drug interactions Glibenclamide
The hypoglycemic effect of glibenclamide is enhanced by the simultaneous use of sulfonamides, PAS, chloramphenicol, fibrates, azapropazone, sulfinpyrazone, coumarin derivatives, miconazole, salicylates, tetracyclines, MAO inhibitors, fenfluramine, pentoxifylline, ACE inhibitors, anabolic steroids, fluoxetine, tritoc valine, cyclophosphamide, ifosfamide, insulin , as well as other antidiabetic drugs (for example, metformin, acarbose). Sympatholytics (β-blockers, reserpine, clonidine), when used continuously, help reduce blood glucose levels, but from a clinical point of view, their ability to weaken or mask the symptoms of hypoglycemia is more important. The hypoglycemic effect of glibenclamide is weakened by barbiturates, phenytoin, rifampicin, glucagon, adrenaline and other sympathomimetic agents, thyroid hormones, corticosteroids, diuretics (including acetazolamide), nicotinic acid in high doses, phenothiazines, diazoxide, as well as sex hormone preparations (gestagens, estrogens) . Alcohol and H2 receptor antagonists can both weaken and enhance the hypoglycemic effect of glibenclamide.
Overdose of the drug Glibenclamide
Symptoms of hypoglycemia occur - hunger, increased sweating, tachycardia, tremor, anxiety, headache, depression, irritability, sleep disturbance, motor coordination, speech and vision, decreased attention, coma. For mild hypoglycemia, consumption of foods rich in glucose and/or sugar is indicated. In case of hypoglycemic coma, concentrated glucose solution (40–100 ml of 20% solution) is administered intravenously, then 5–10% glucose solution is infused, and 1–2 mg is also administered intramuscularly or subcutaneously glucagon. To prevent relapses of hypoglycemia over the next 24–48 hours, carbohydrates are prescribed orally (20–30 g immediately, and then every 2–3 hours) or a long-term infusion of glucose is performed (5–20% solution); You can administer 1 mg of glucagon intramuscularly over 48 hours every 6 hours. After severe hypoglycemia, blood glucose levels are regularly monitored for 48 hours. In case of acute poisoning, suicide attempt and prolonged coma, gastric tube lavage and administration of an aqueous suspension of activated carbon are performed. A long-term infusion of 5–10% glucose solution is prescribed. After 20 minutes, it is possible to re-inject concentrated glucose solution. Glibenclamide is not excreted from the body during hemodialysis.
List of pharmacies where you can buy Glibenclamide:
- Moscow
- Saint Petersburg
Glibenclamide
The hypoglycemic drug glibenclamide, in its chemical structure, belongs to the 2nd generation of sulfonylurea derivatives. Despite all the pharmaceutical “decrepitness” of this drug (and it has been used in clinical practice since 1969), its reliability and knowledge allow it to stay afloat to this day. And not just to be somewhere in the margins, but to be one of the most popular means for treating type 2 diabetes. In laboratory and clinical trials, glibenclamide is still the standard for evaluating the effectiveness of new pharmacologically active substances and approaches in antidiabetic therapy, while demonstrating new beneficial properties. The mechanism of the hypoglycemic activity of glibenclamide, as well as other drugs in this group, has been studied in the most detail, literally disassembled into molecules: the drug blocks the potassium channels of pancreatic β-cells, which automatically promotes the entry of calcium ions into the cell, which in turn cause the destruction of insulin granules and release of the latter into the blood and intercellular fluid. Among all sulfonylurea derivatives, glibenclamide is endowed with the most pronounced affinity for the corresponding receptors on β-cells and the strongest hypoglycemic effect among all sulfonylurea derivatives. The greater the dose of the drug taken, the more massive the release of insulin. All drugs of this class also have so-called extrapancreatic effects, making peripheral tissues more sensitive to insulin and improving the absorption of glucose by adipose and muscle tissues.
This circumstance contributes to additional absorption of glucose by tissues (read: decreased glycemia).
Thus, glibenclamide still remains competitive according to a number of criteria. First of all, it is effective, proven by many years of practice. The drug prevents the long-term consequences of diabetes mellitus, including myocardial infarction and microvascular complications. Glibenclamide is successfully combined with other drugs, for example, metformin, and if disease compensation is not achieved, good results can be obtained from the triple combination of metformin + glibenclamide + glitazone. Glibenclamide is successfully used in elderly patients with a “bouquet” of concomitant diseases. And what is important (and for many of our compatriots - most important), the drug is accessible from a socio-economic point of view. It is cheaper than many of its more modern “comrades” in the fight against diabetes.
When taking glibenclamide, it is necessary to carefully monitor glucose levels due to the potential risk of hypoglycemic reactions. If a patient who has taken the drug is “covered” by hypoglycemia, then it is necessary to immediately ensure that glucose enters his body (orally or by injection, depending on his state of consciousness). As an option, keep foods rich in fast carbohydrates on hand at all times.